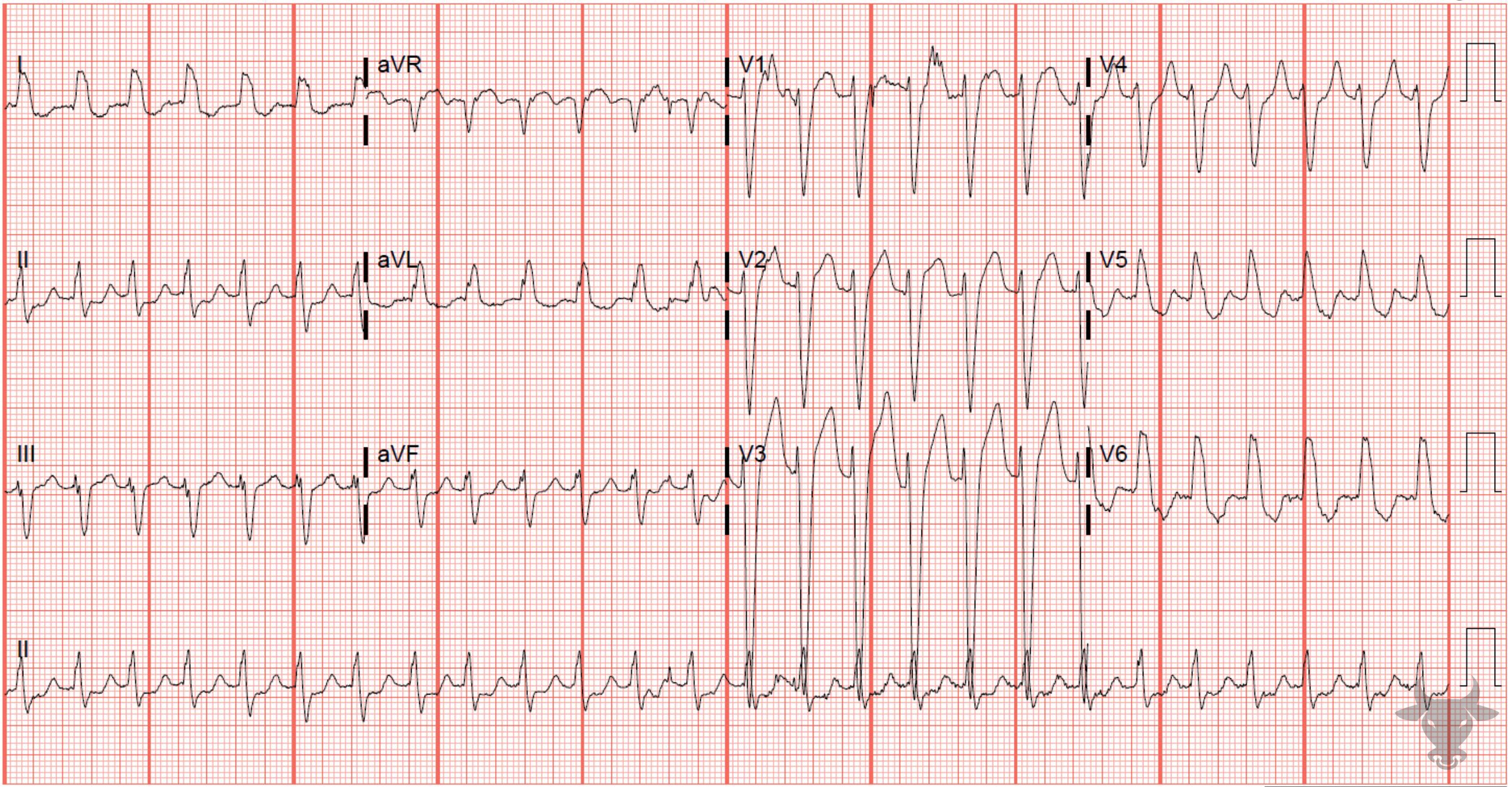
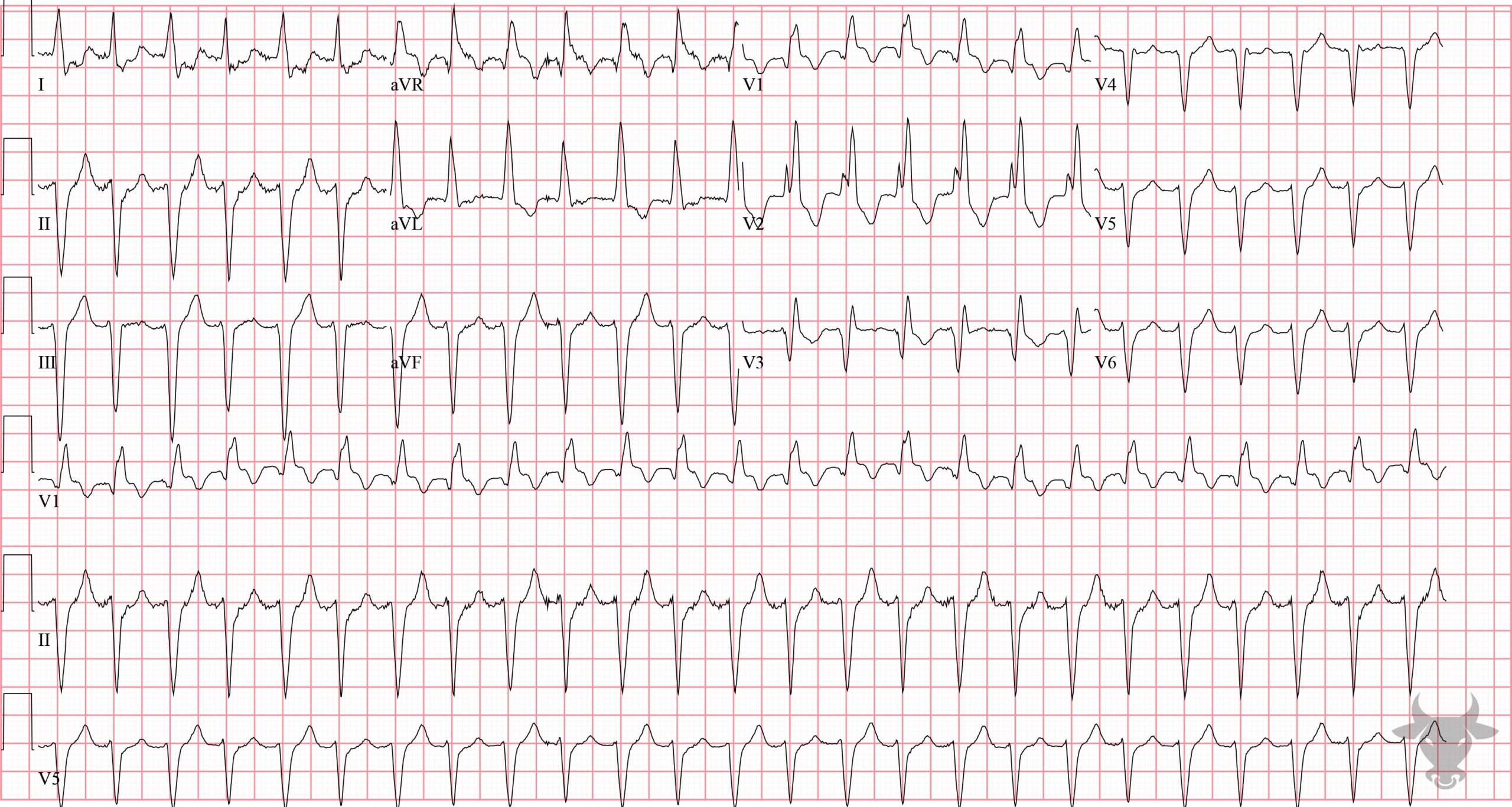
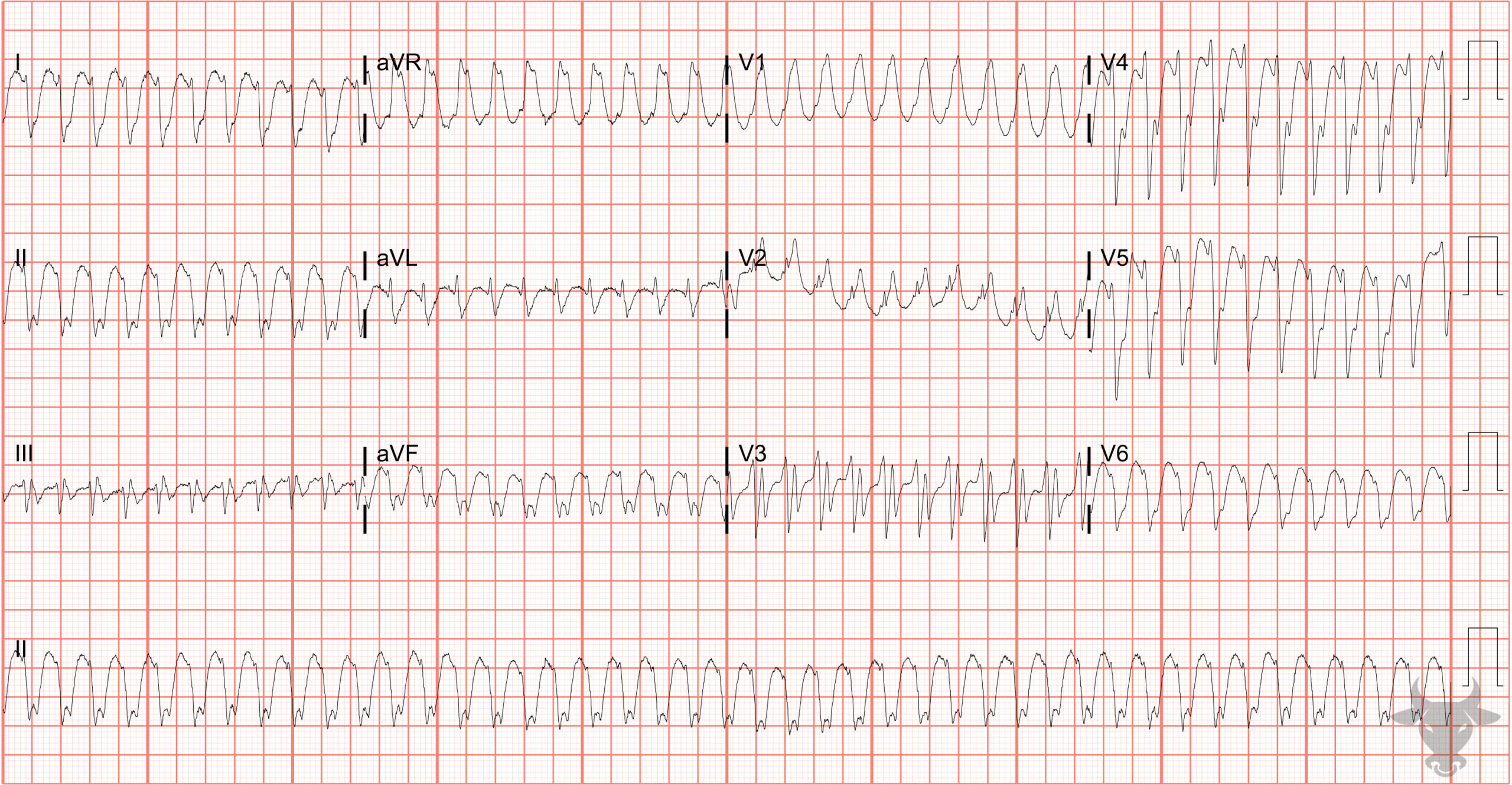
The differential for wide complex tachycardia includes ventricular tachycardia (VT), supraventricular tachycardia (SVT, e.g., atrial flutter, atrial tachycardia, or atrioventricular nodal reentrant tachycardia) with aberrancy (i.e., bundle branch block), antidromic atrioventricular reentrant tachycardia, and toxicologic/metabolic disturbances (e.g., sodium-channel blockade, hyperkalemia). There are obvious perils of missing VT, and the test characteristics of the various criteria for differentiating VT vs SVT with aberrancy may be insufficient given the serious implications of falsely diagnosing SVT. Therefore, unless there is a compelling alternative, VT should be assumed.
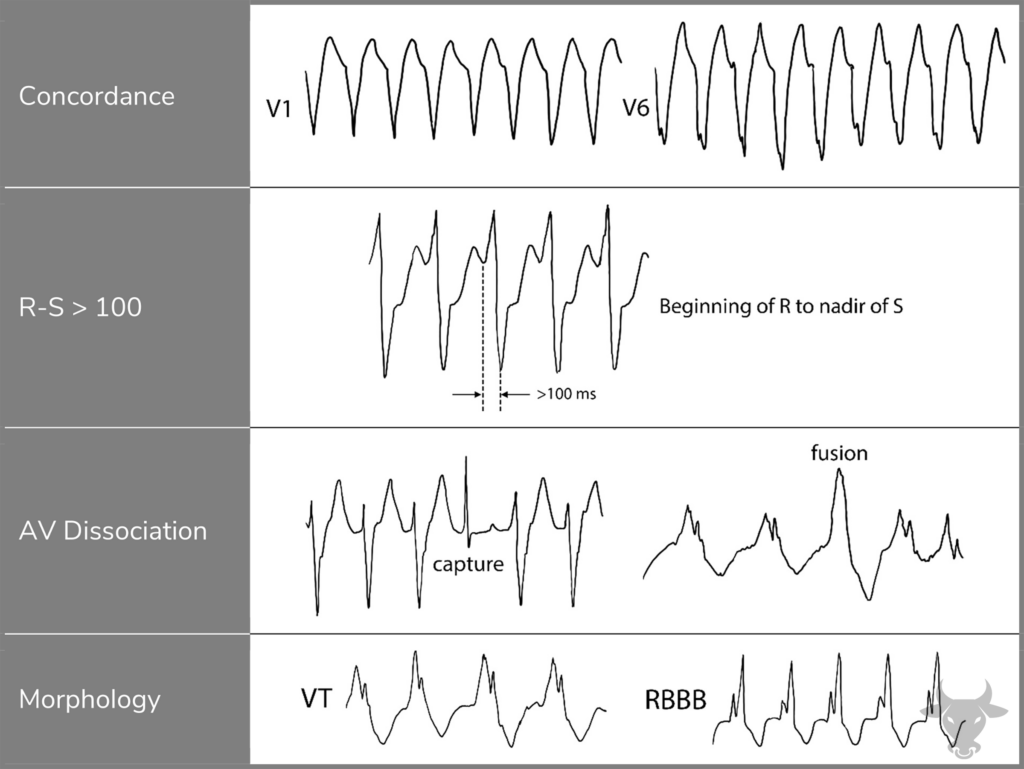
These features are adapted from the Brugada algorithm, which is one of several algorithms to help differentiate between supraventricular tachycardia with aberrancy and ventricular tachycardia. If any condition is met, ventricular tachycardia is diagnosed. Concordance describes QRS complexes in the same direction (up or down) across the precordium (V1 – V6). Signs of AV dissociation include capture beats, fusion beats, or occasionally P waves can be visualized. If the previous three criteria are not met and the morphology suggests aberrancy, then ventricular tachycardia is unlikely. Rsr’ appearance (as opposed to rsR’) in V1 strongly favors ventricular tachycardia. AV, atrioventricular.