Classily, sodium channel toxicity was described in tricyclic overdoses,96 but many drugs can cause toxic sodium channel effects including antiarrhythmics (e.g., lidocaine, phenytoin, propafenone, flecainide, amiodarone, sotalol), antiepileptic medications (e.g., carbamazepine, lamotrigine), selective serotonin reuptake inhibitors (e.g., citalopram, fluoxetine), antihistamines (e.g., diphenhydramine), propranolol, cyclobenzaprine, and others. ECG features include a widened QRS, prolonged QT, right axis deviation, tall terminal R in aVR. Patients with sodium channel toxicity need a sodium load. One of the most effective ways of delivering sodium is via 8.4% sodium bicarbonate, which has the dual effect of loading with extracellular sodium and alkalinizing the serum pH, favoring the neutral (i.e., non-ionized) form of the drug and making it less available to bind to sodium channels. Give 1-2 ampules of 8.4% sodium bicarbonate and repeat the ECG, continue until the QRS is < 100 ms to reduce the risk of seizures and arrythmias.
Sodium Channel Toxicity

Examples
Sodium Channel Toxicity
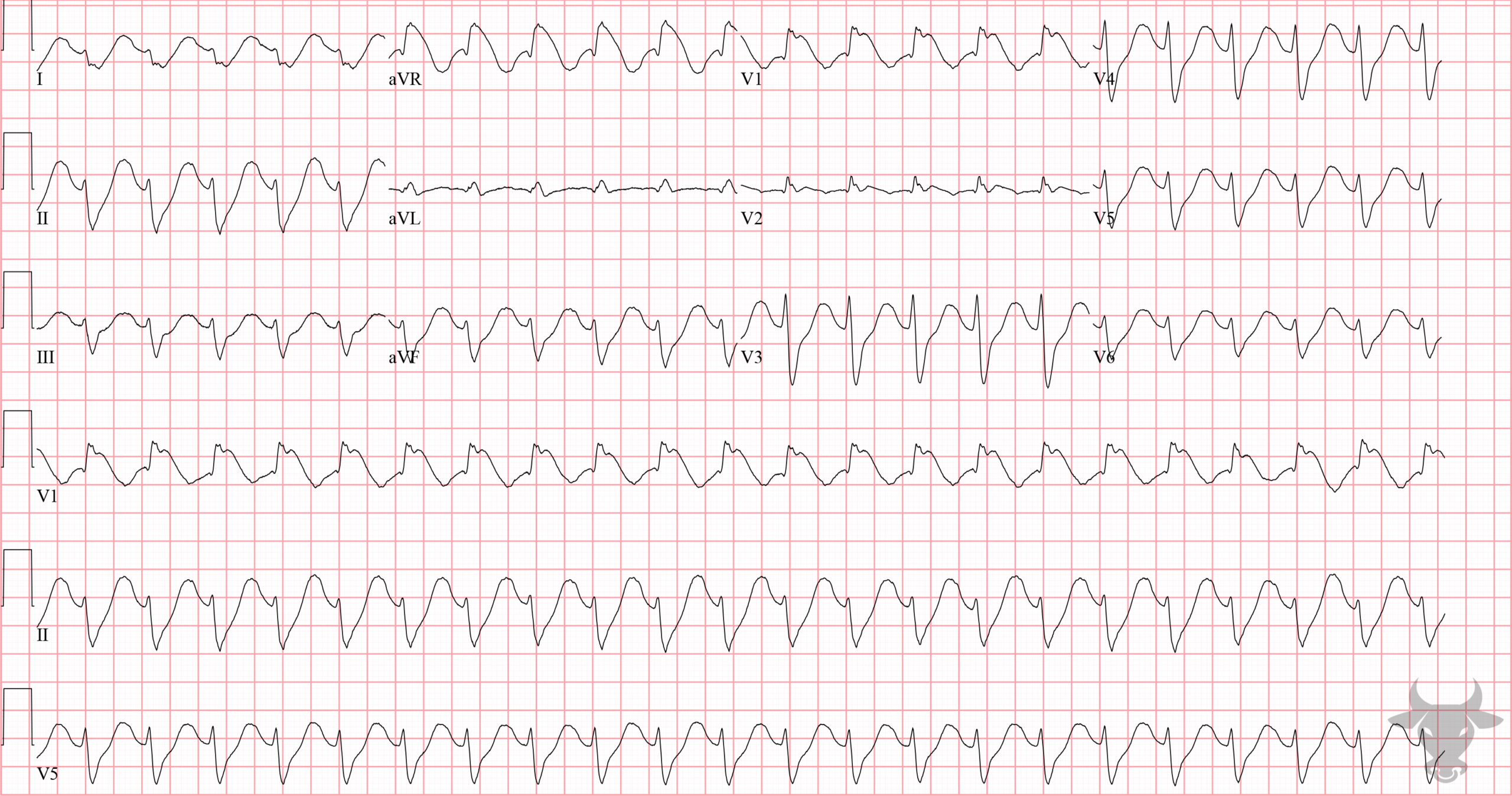
Sodium channel toxicity from a tricyclic antidepressant overdose with right axis deviation, tall terminal R wave in aVR, and widened QRS.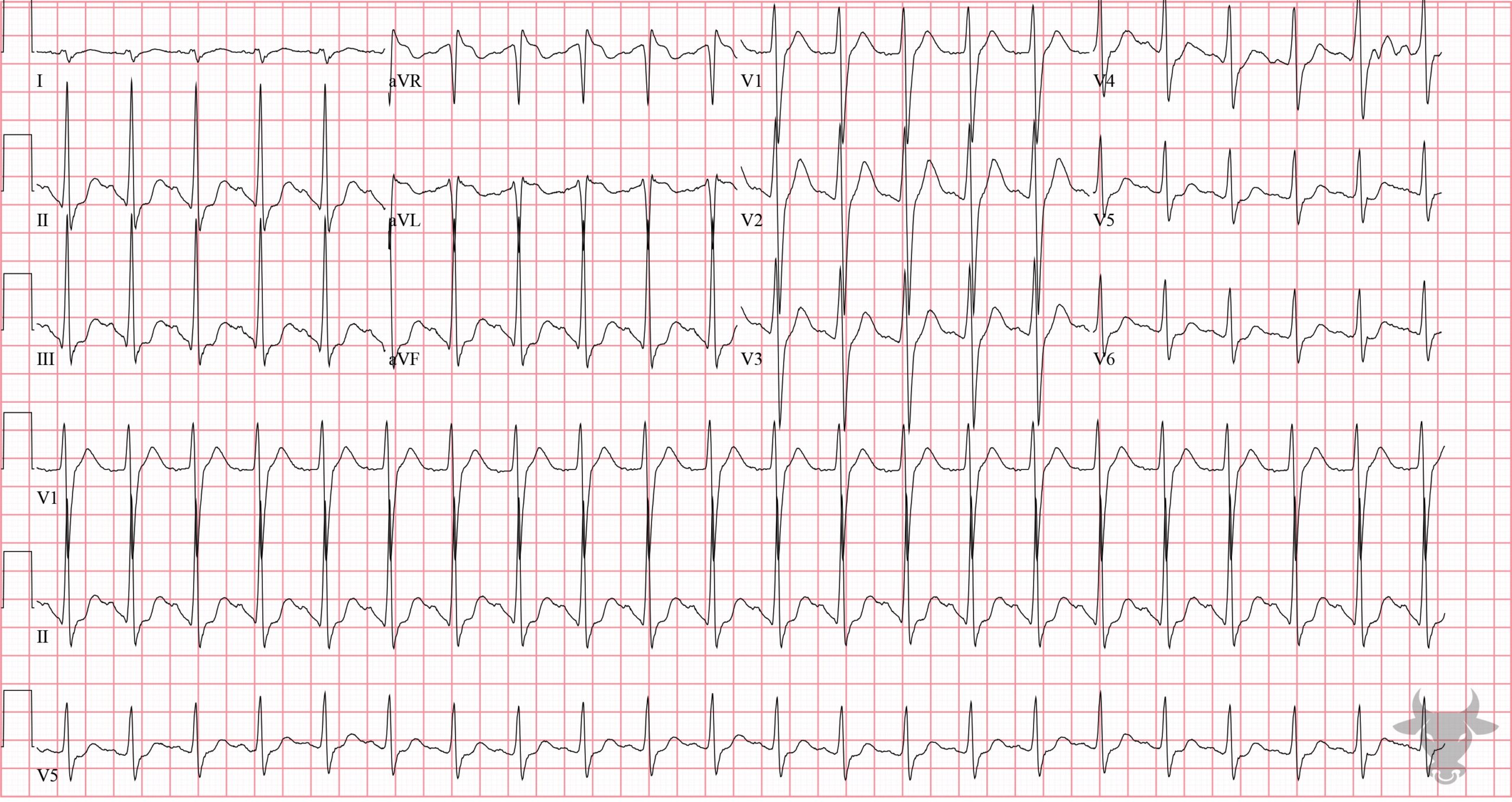
Sodium Channel Toxicity
Sodium channel toxicity from a tricyclic antidepressant overdose. Note the right axis deviation, the tall terminal R wave in aVR, and the widened QRS.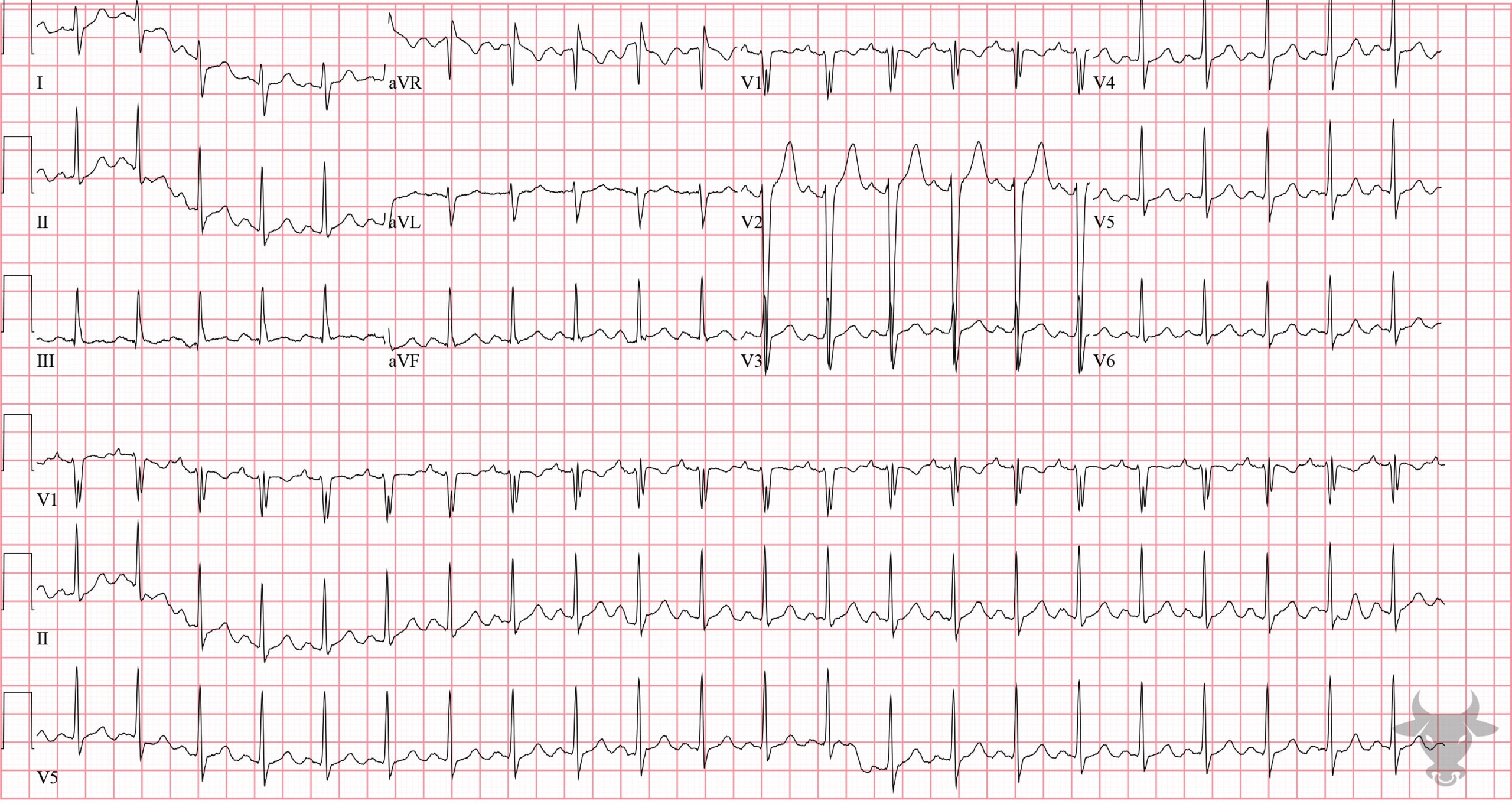
Sodium Channel Toxicity
Tricyclic antidepressant overdose. Note the right axis deviation, tall terminal R wave in aVR, and the slightly widened QRS complex.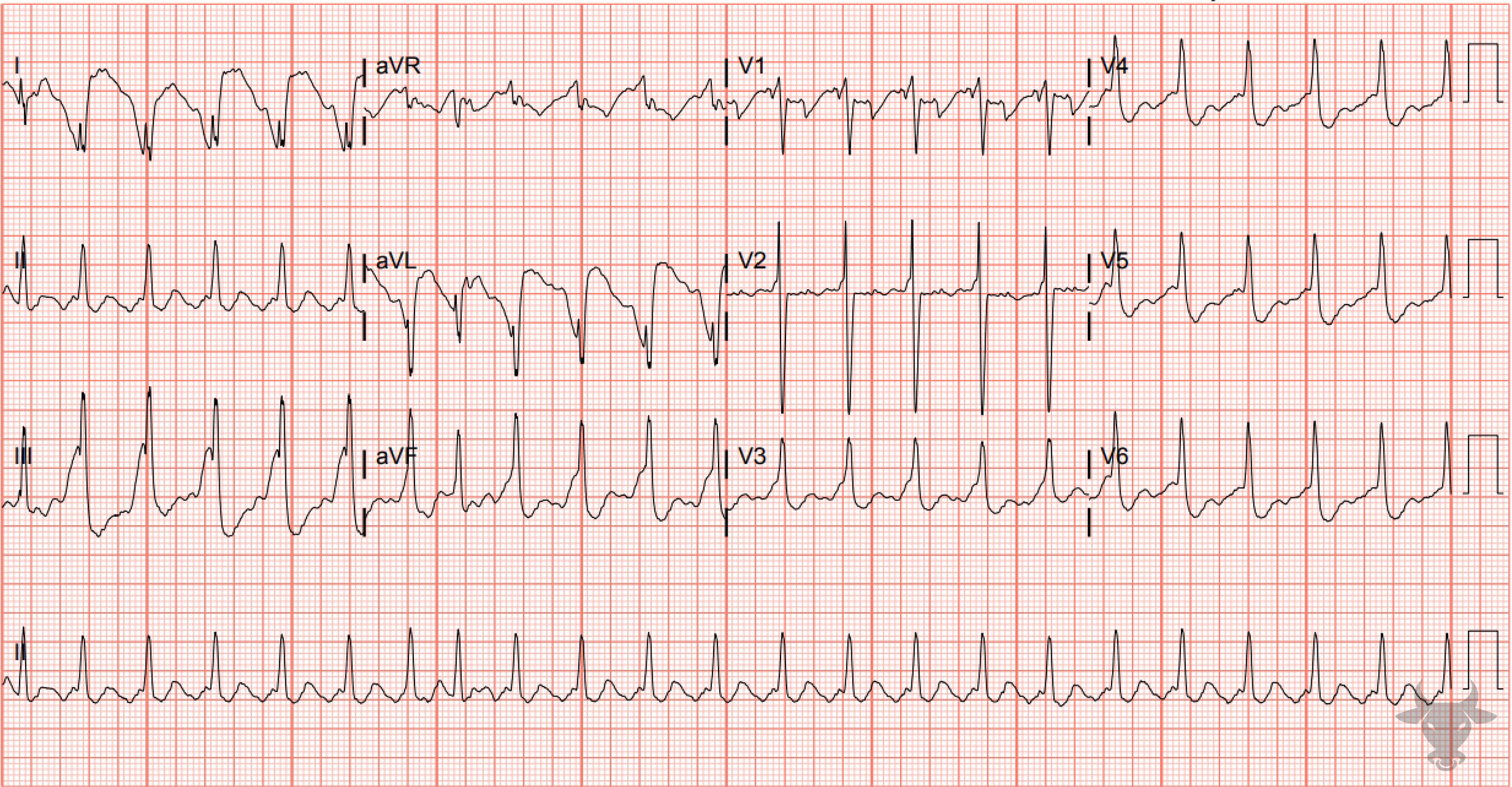
Sodium Channel Toxicity
Atrial flutter with 2:1 conduction. The wide and fragmented QRS, right axis deviation, and tall terminal R wave in aVR are all consistent with sodium channel toxicity; in this case, due to cocaine toxicity.References
- Boehnert MT, Lovejoy FH. Value of the QRS duration versus the serum drug level in predicting seizures and ventricular arrhythmias after an acute overdose of tricyclic antidepressants. New England Journal of Medicine. 1985;313(8):474-479.
- Gray A, Talari G, Mirrakhimov AE, Barbaryan A, Ayach T, Chadha R. The Role of Sodium Bicarbonate in the Management of Some Toxic Ingestions. International Journal of Nephrology. 2017;2017:1-8.
- Kerr GW, Mcguye AC, Wilkie S. Tricyclic antidepressant overdose: a review.