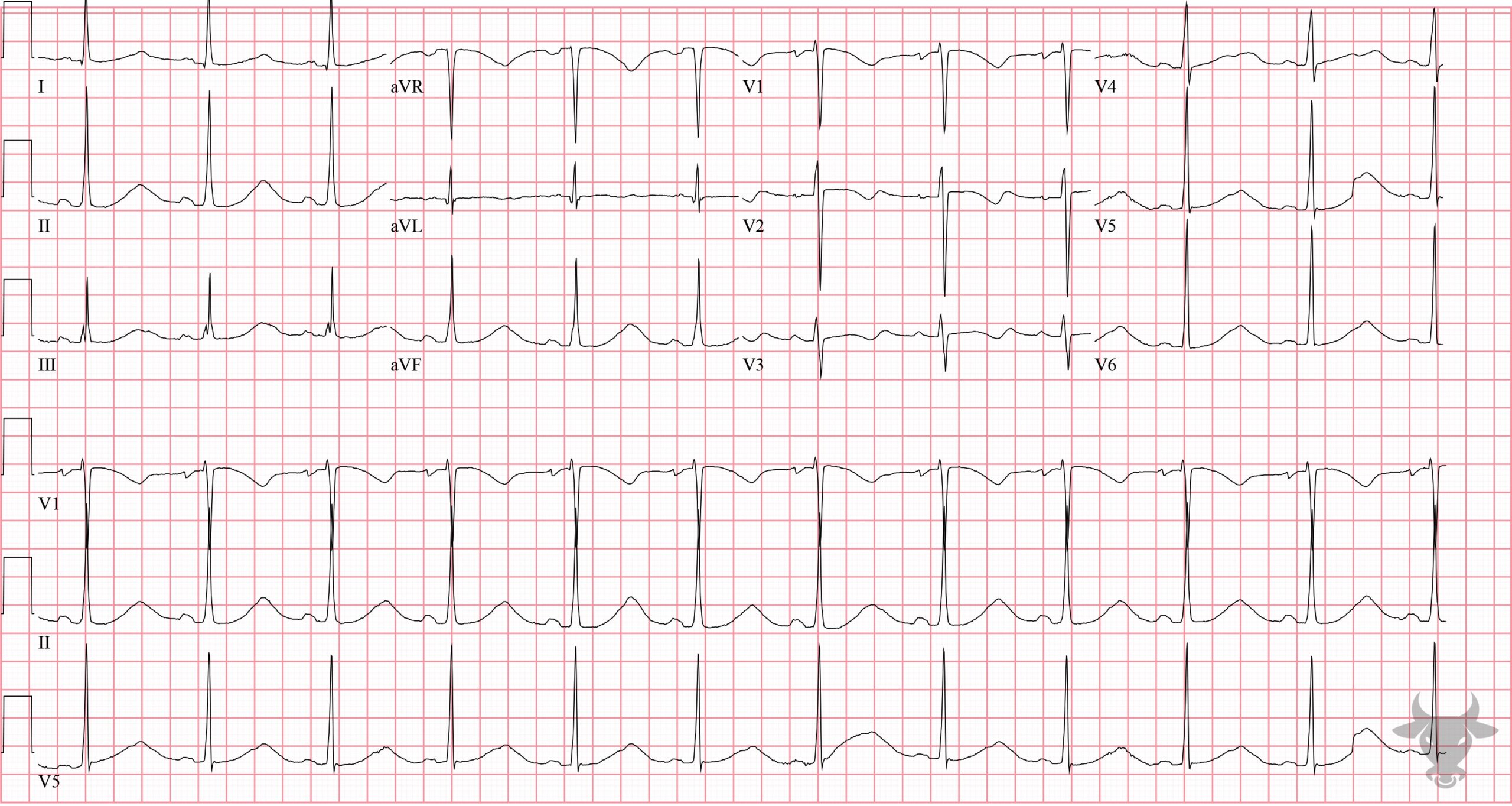
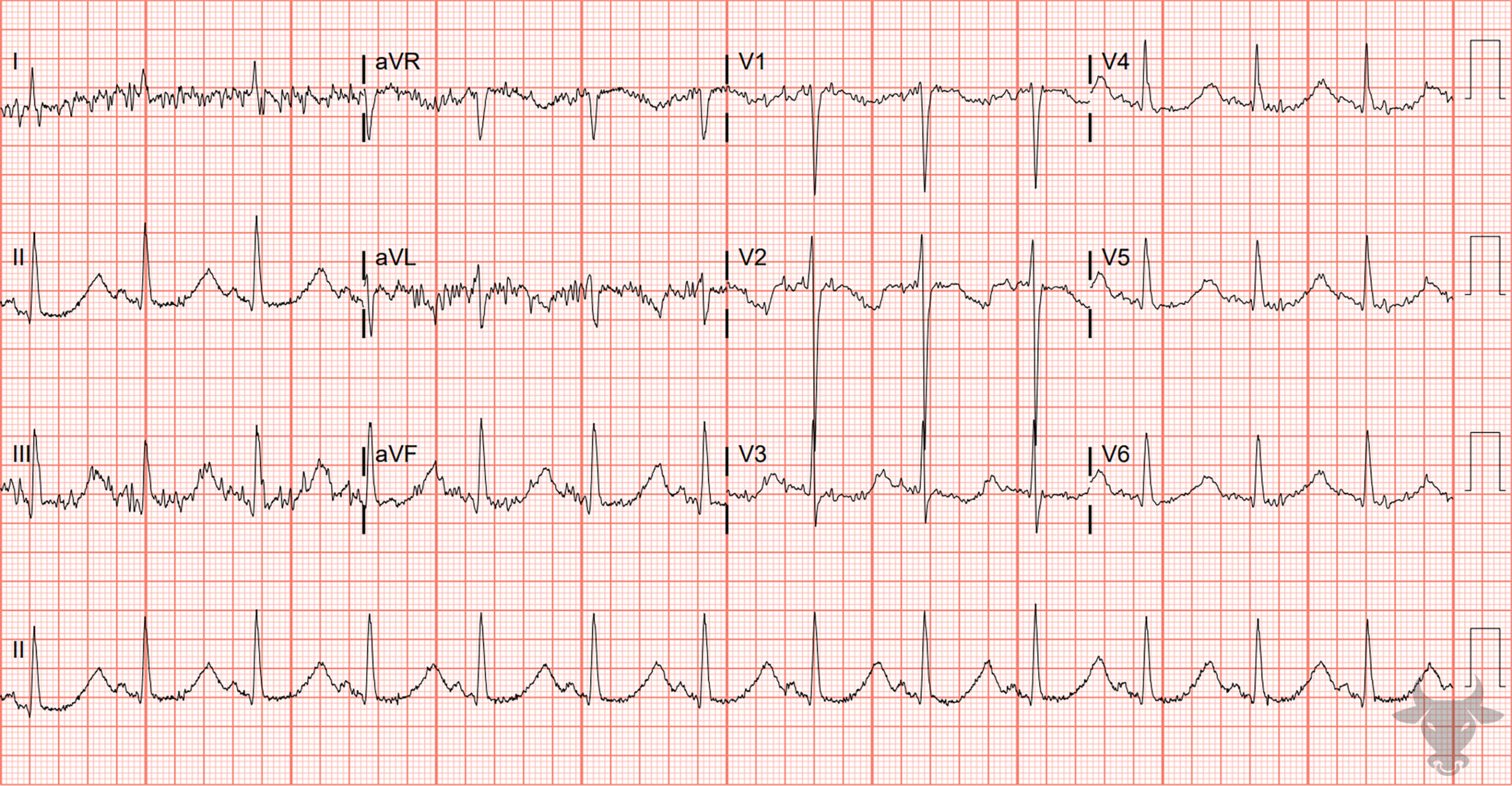
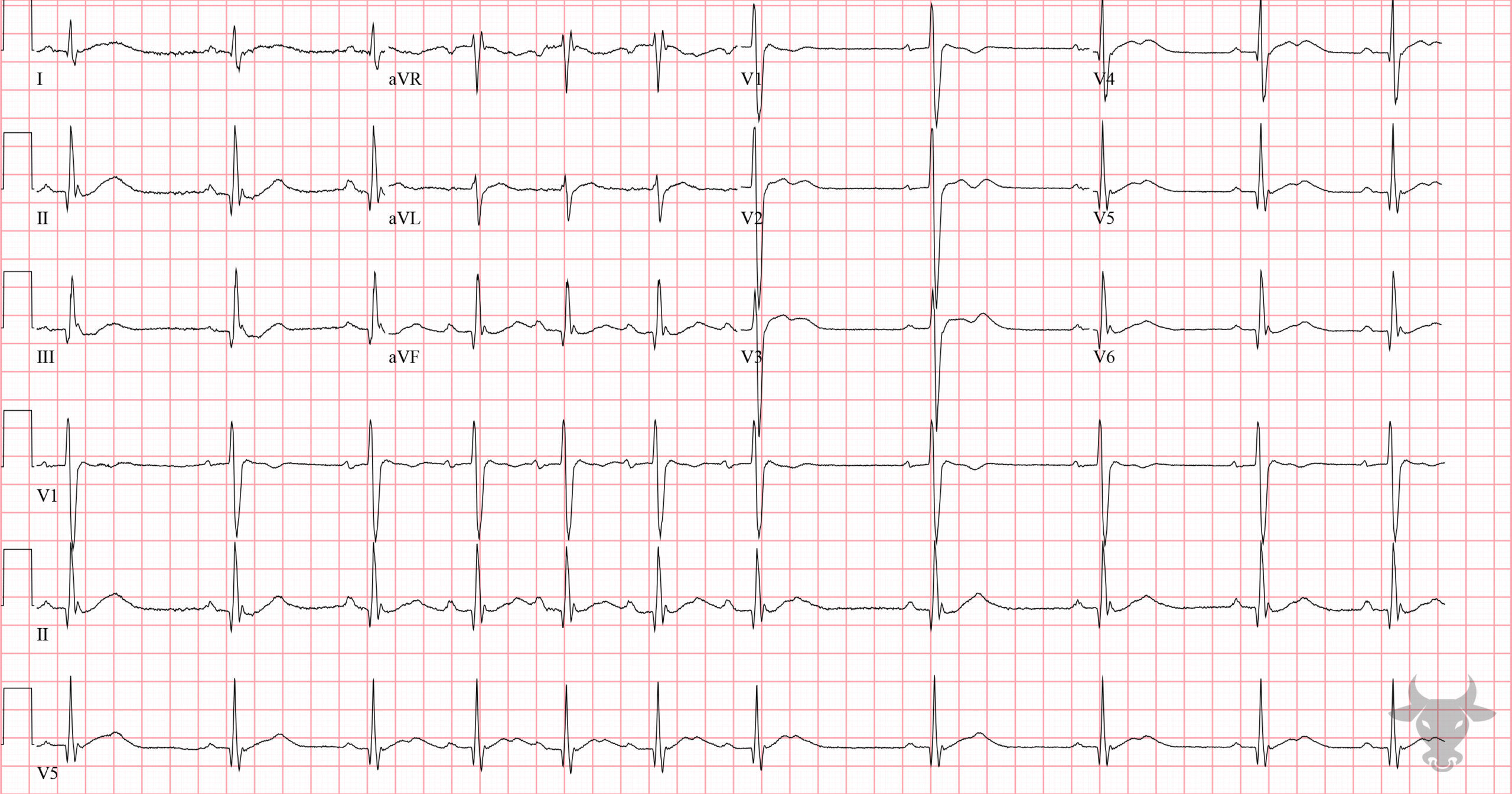
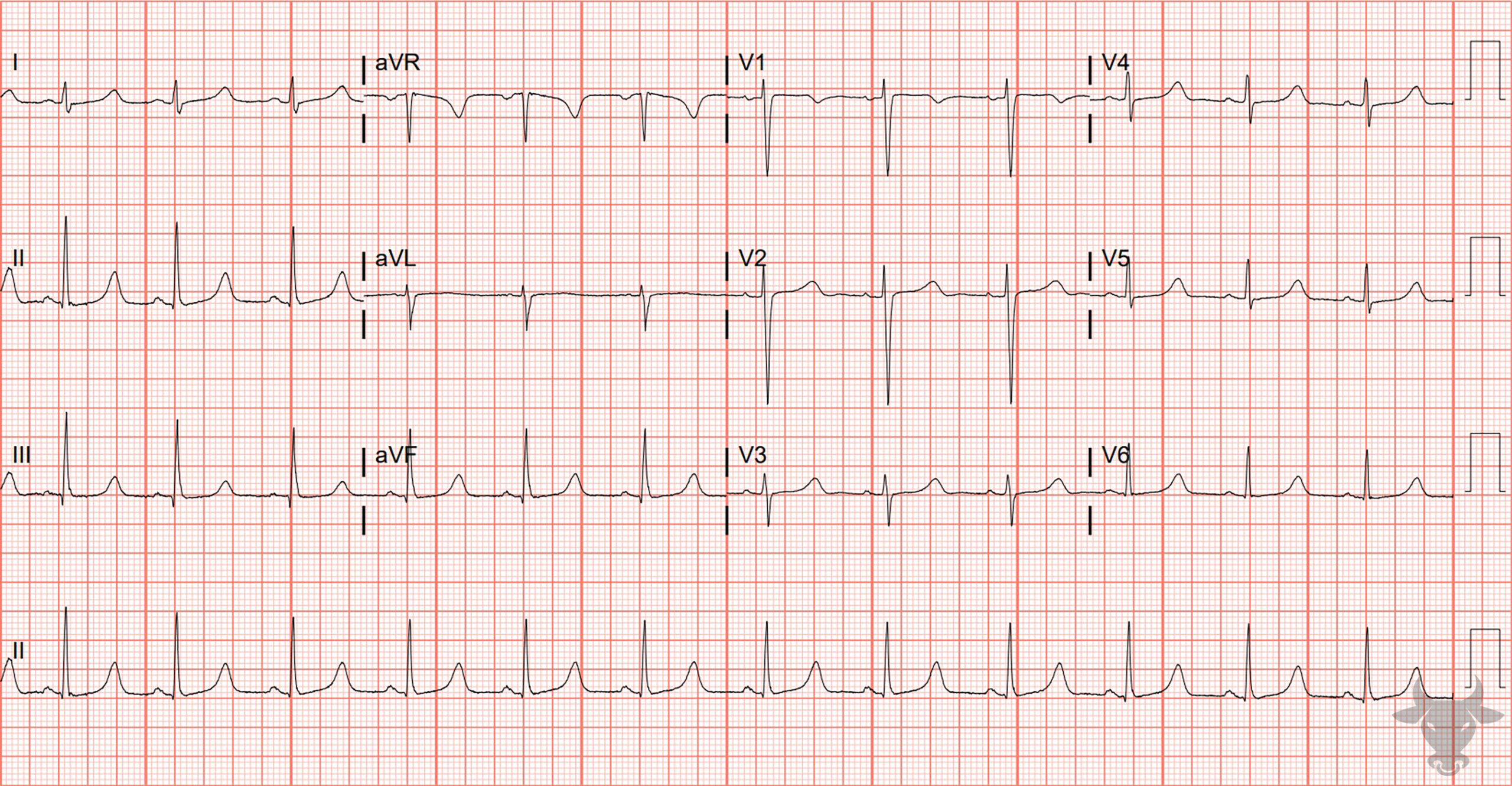
Measuring the QT can be challenging, and many different methods exist. One simple method is the “half the RR” rule – the QT interval is prolonged if it occupies more than half the R-R interval. The “half the RR” rule is a conservative estimate at normal and tachycardic rates, but perhaps a better option at bradycardic rates is an absolute cut-off of 485 ms. Causes of long QT include congenital cardiac ion channel mutations (i.e., Na or K channelopathies), electrolyte imbalance (i.e., hypokalemia, hypomagnesemia, hypocalcemia), medications (e.g., amiodarone, tricyclic antidepressants, methadone, antibiotics, ondansetron, antipsychotics, and many, many others), hypothermia, and hypothyroidism. Prolonged QT places someone at risk of developing Torsades de Pointes due to early afterdepolarizations/triggered activity during the repolarization phase (i.e., R on T phenomenon). Torsades de pointes is an unstable polymorphic ventricular tachycardia characterized by QRS complexes that “twist” around the isoelectric line.

Torsades de Pointes.