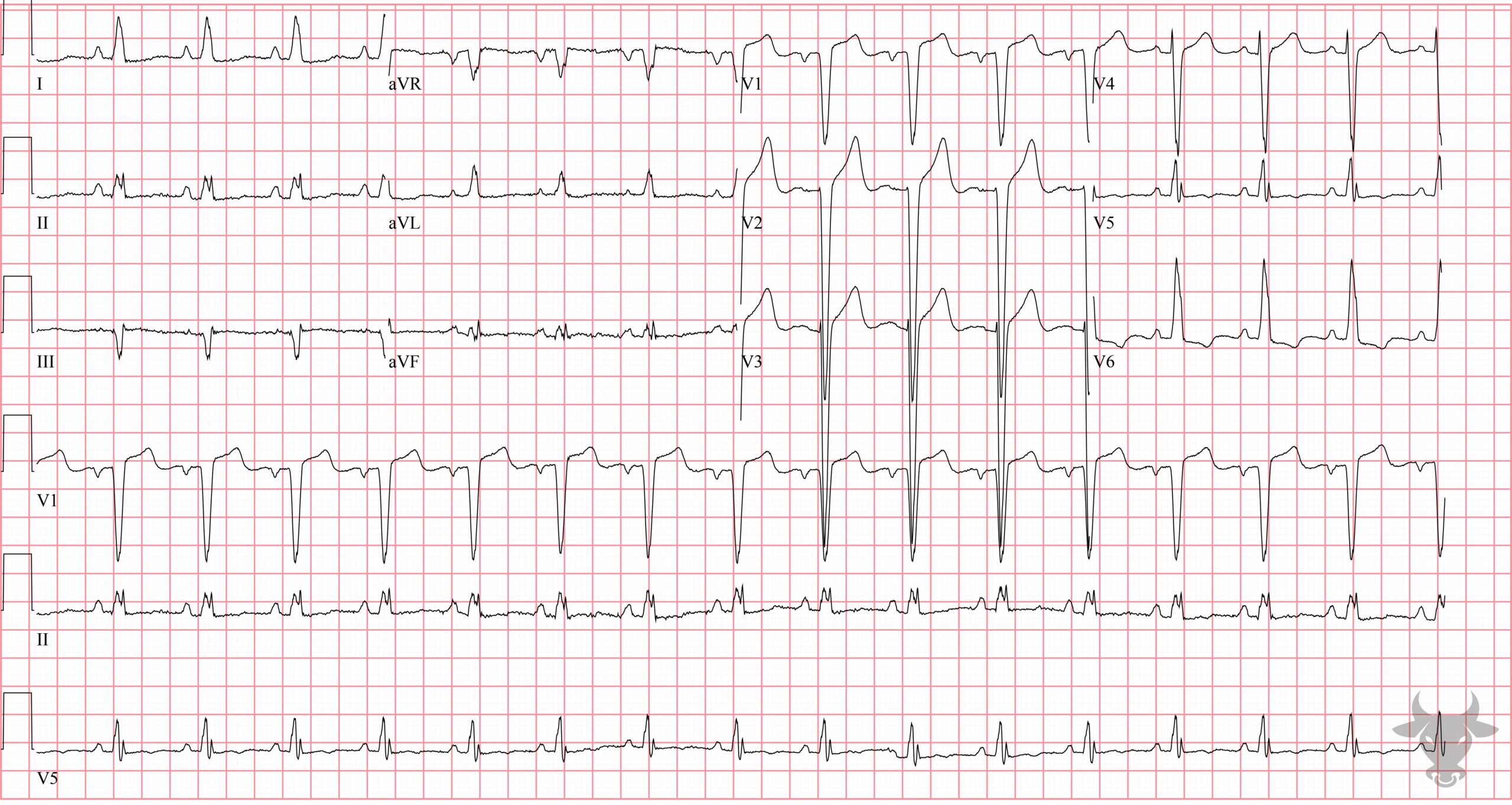
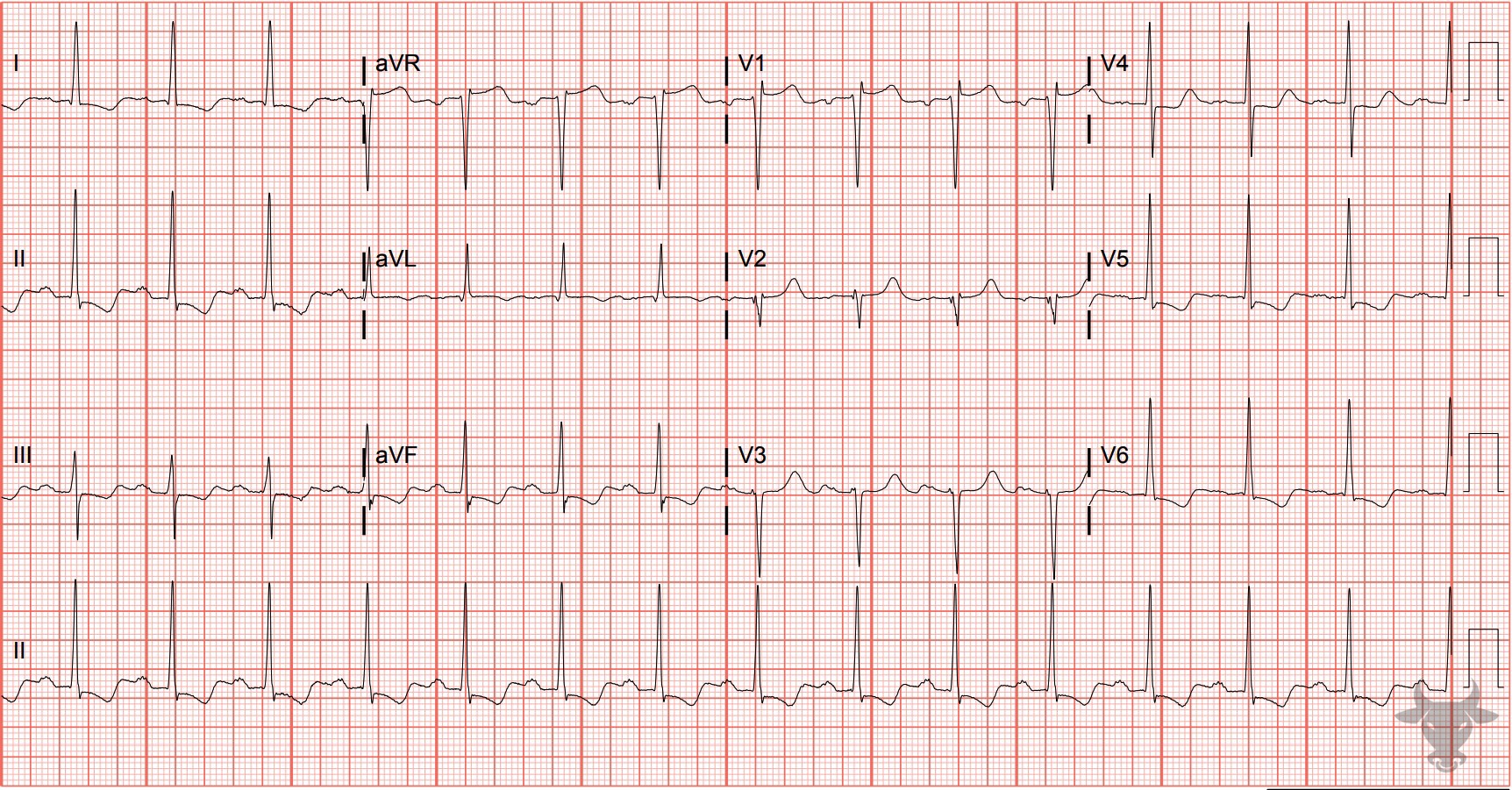
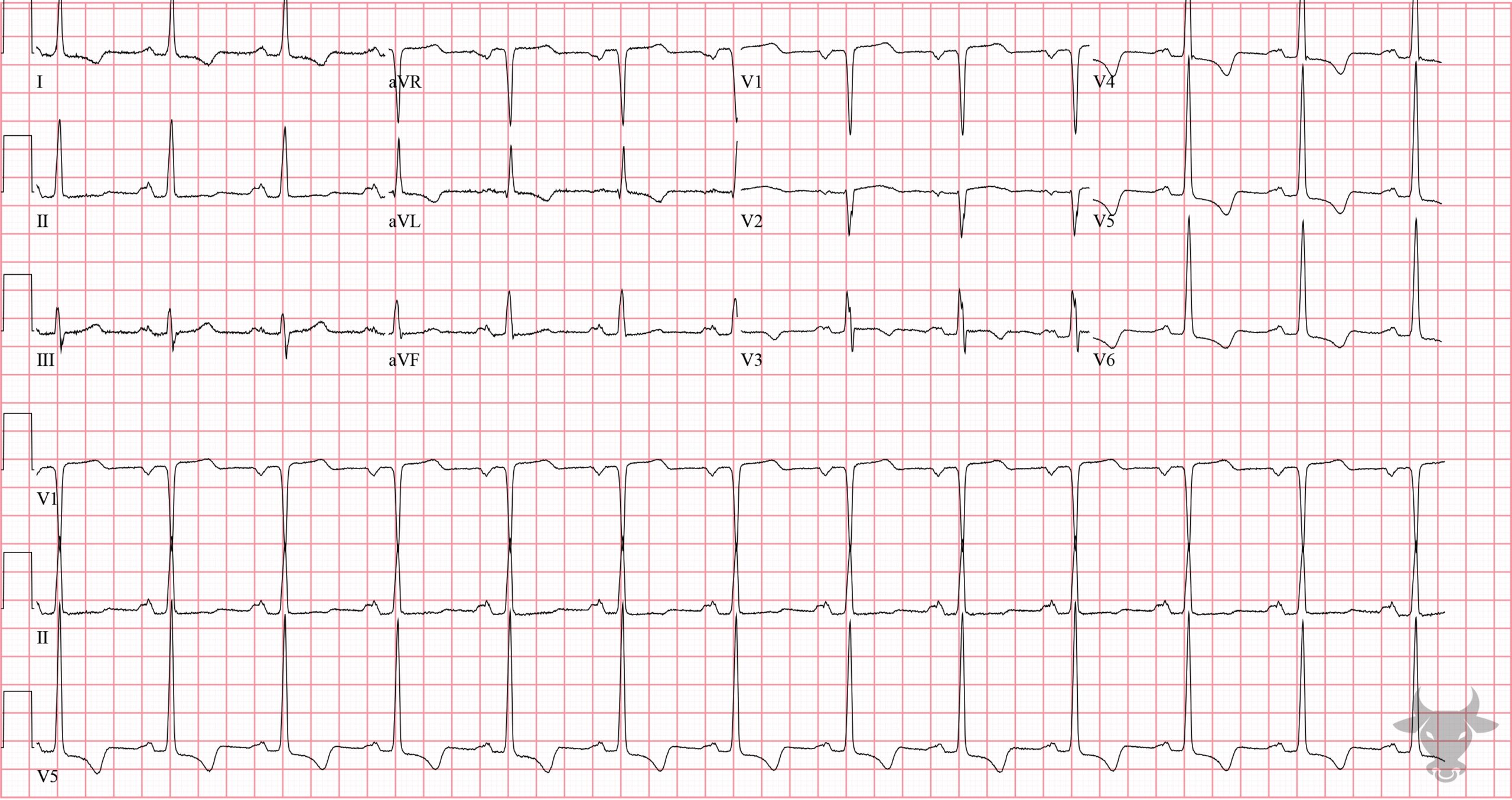
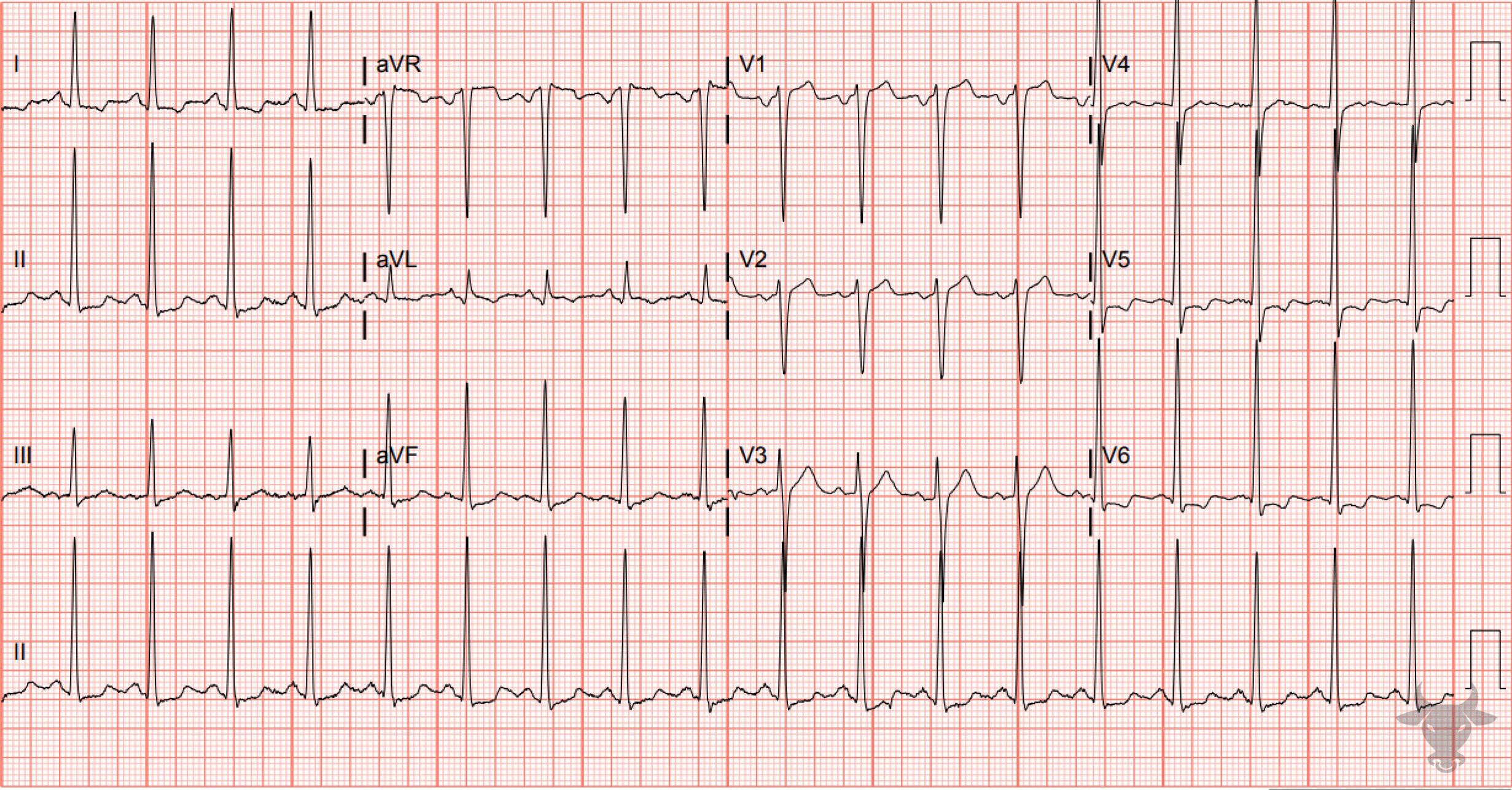
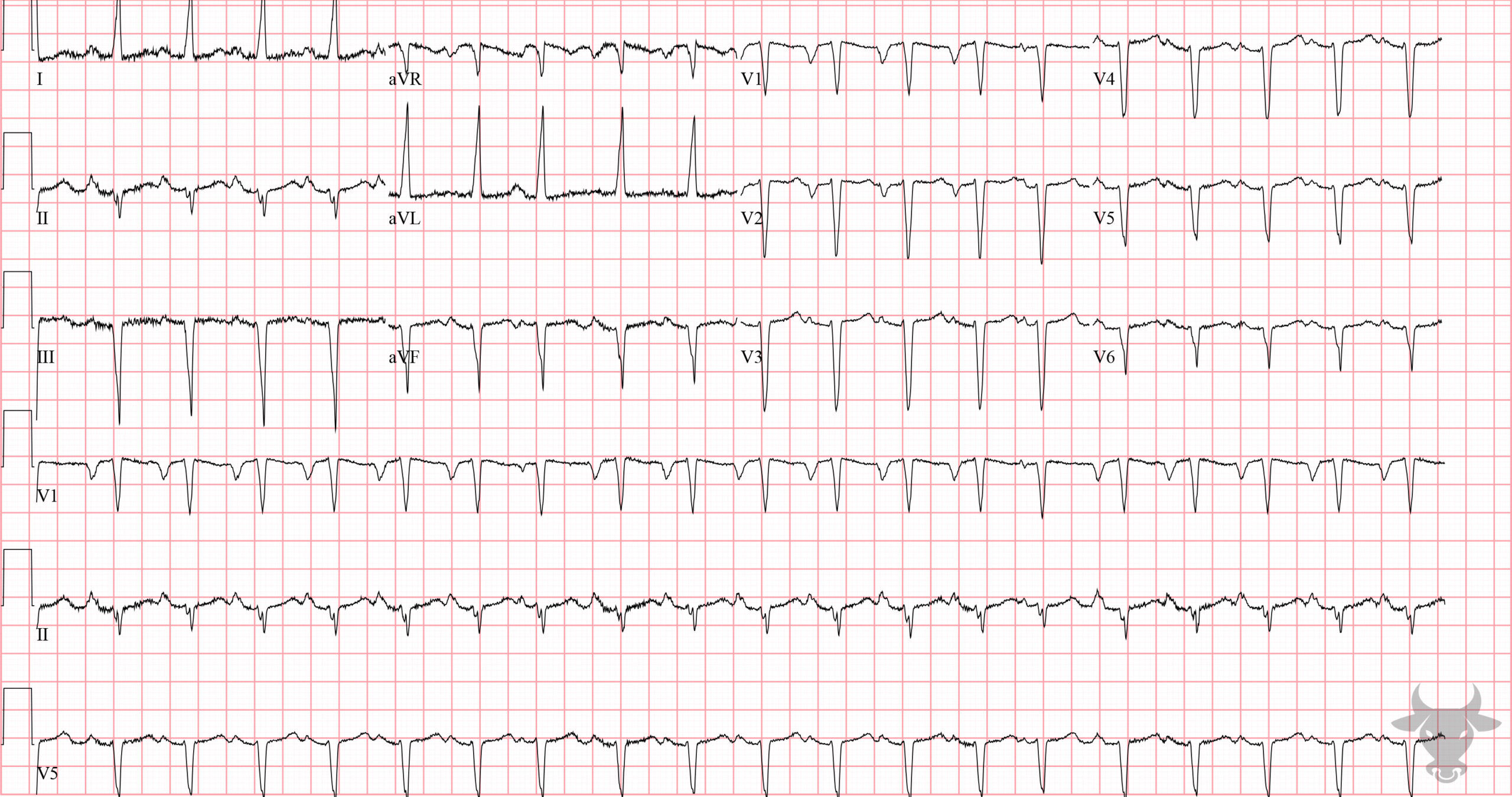
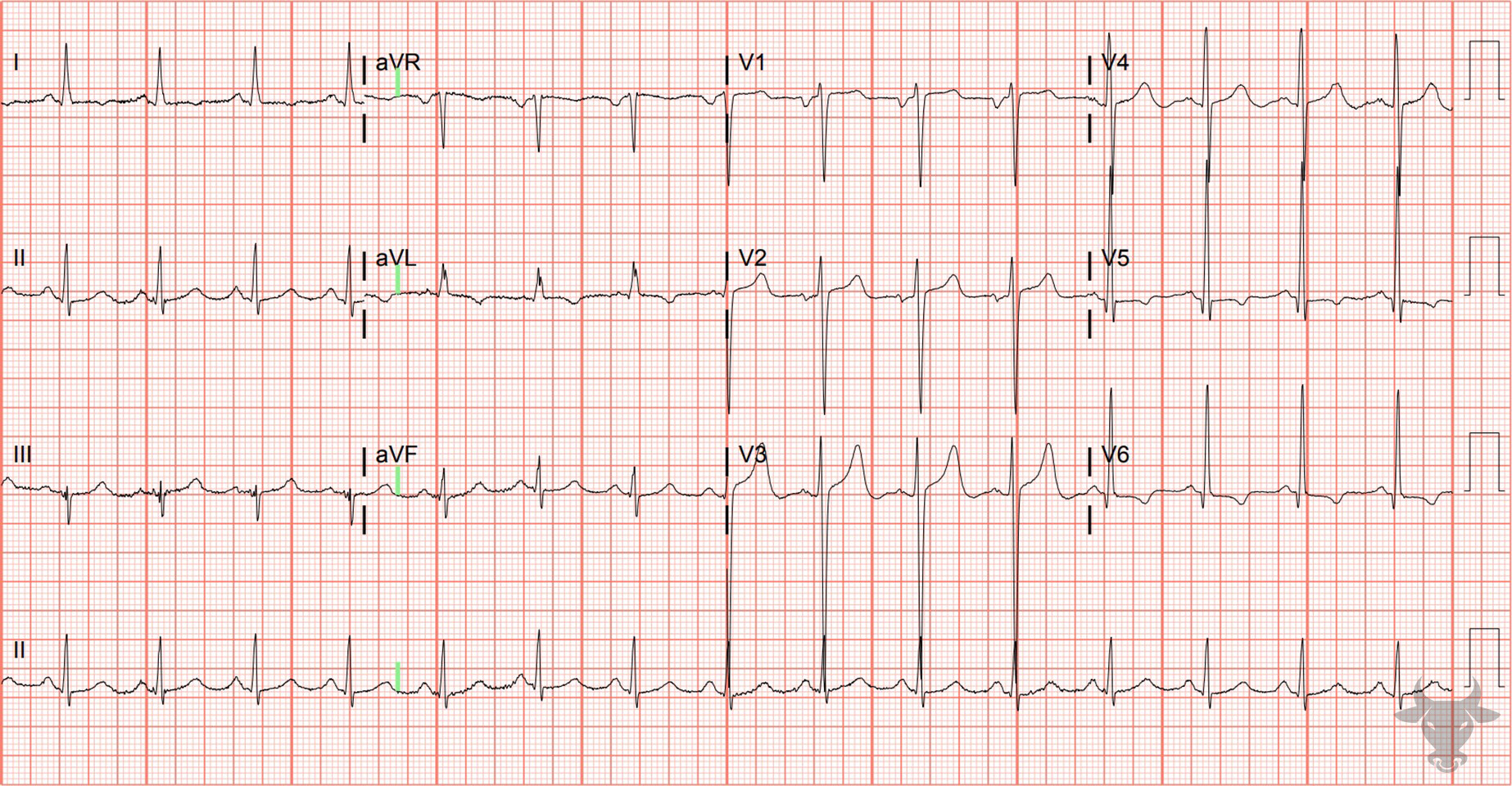
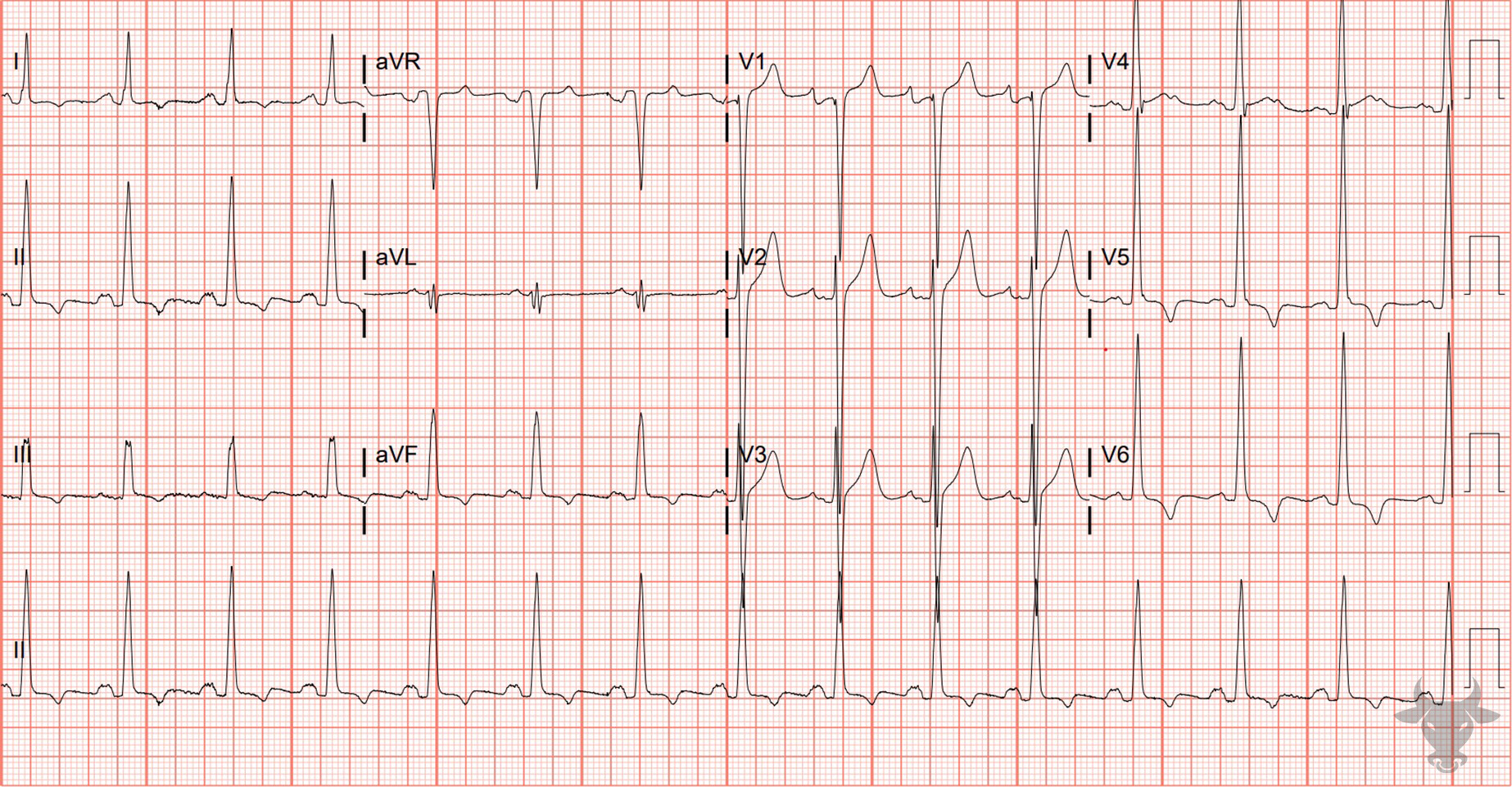
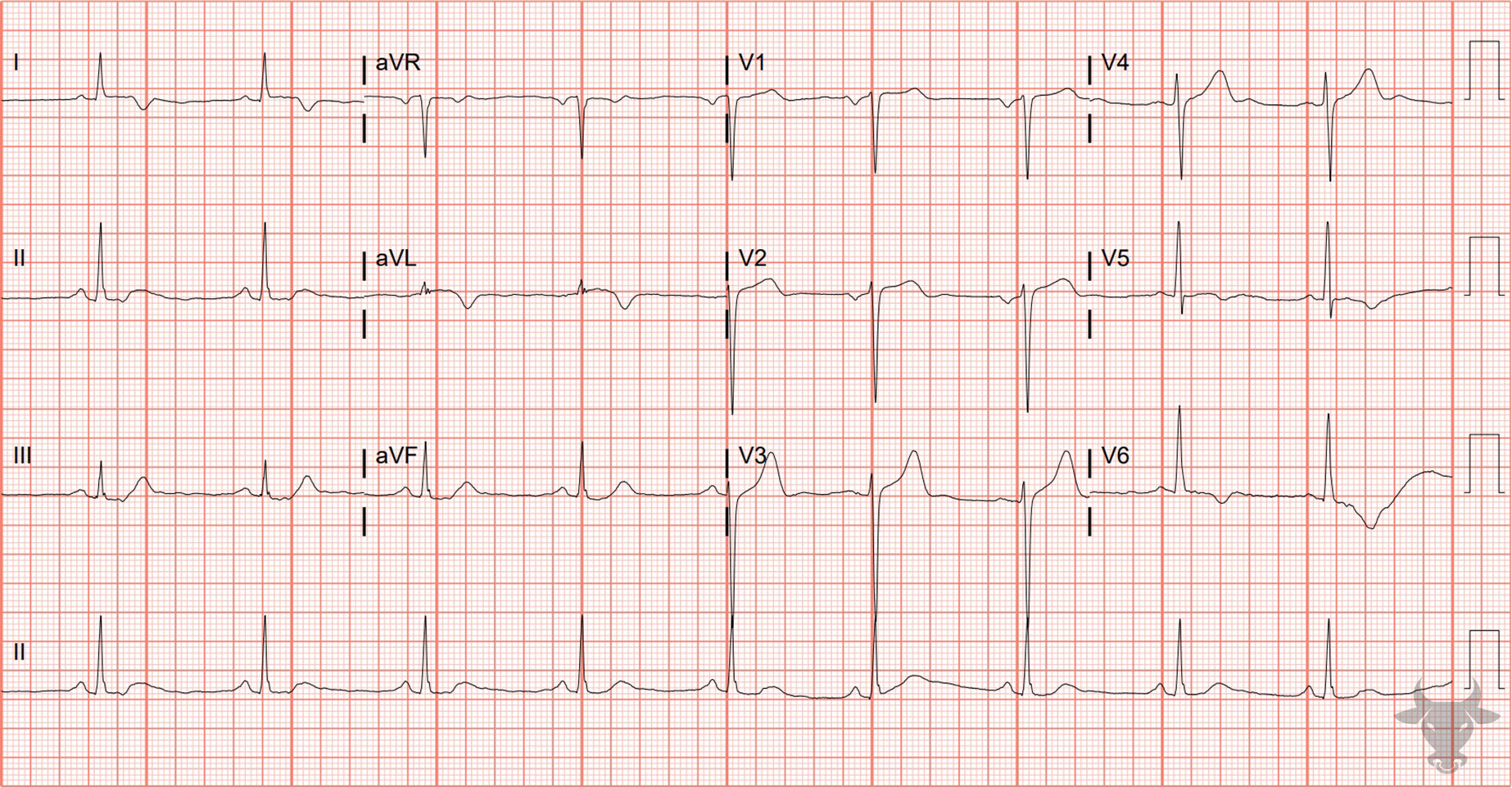
There are several criteria out there for left ventricular hypertrophy, and none of them are particularly sensitive. They’re all less than 50% sensitive, but they’re usually quite specific – 85 to 90%. The most cited criteria are the Sokolow-Lyon and the Cornell criteria, which consider voltage amplitude. There are also ST/T wave changes associated with LVH that may increase the specificity when seen. Namely, lateral ST depressions and asymmetric T wave inversions.

Select electrocardiographic criterial for Left ventricular hypertrophy.
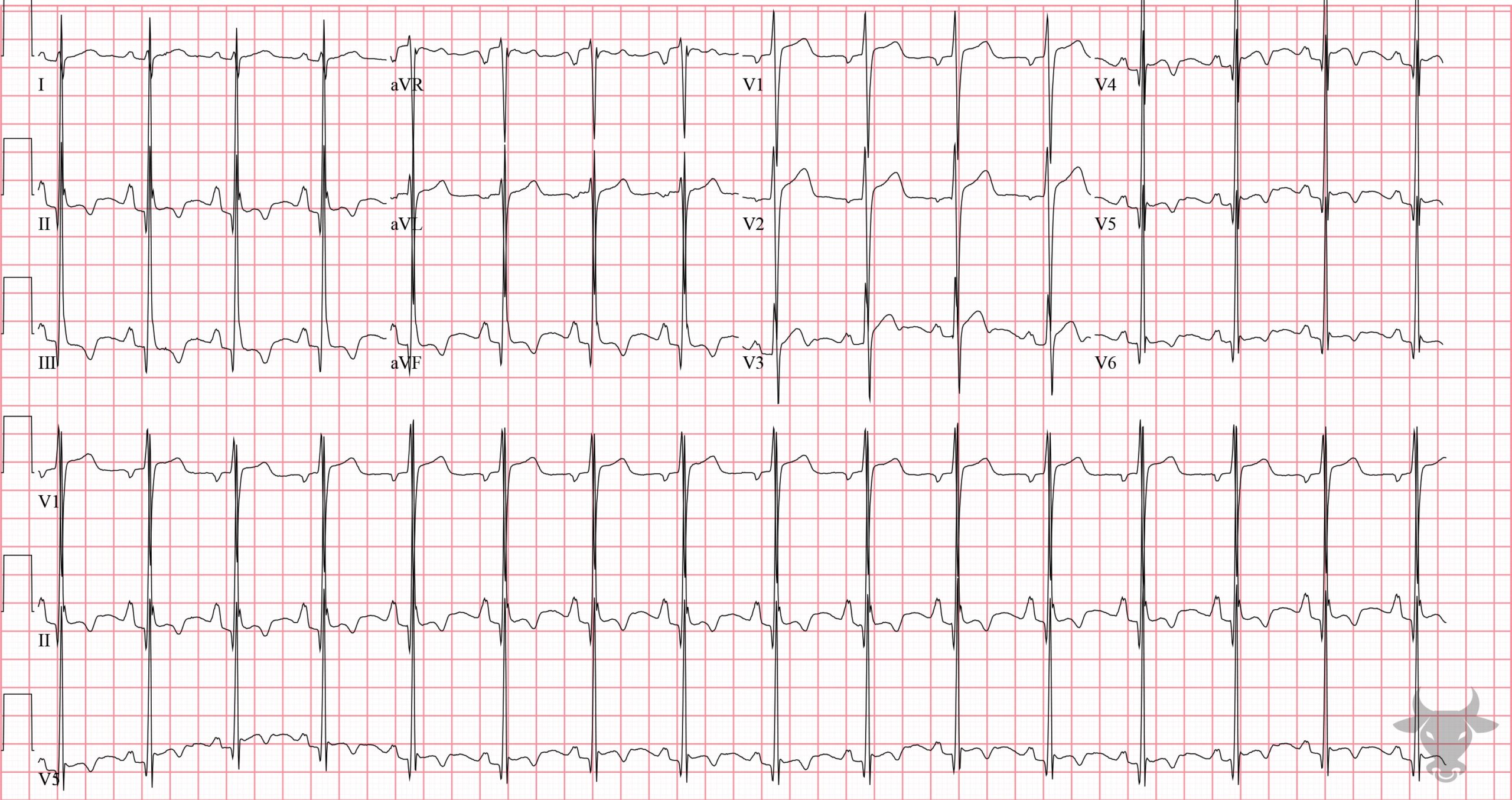
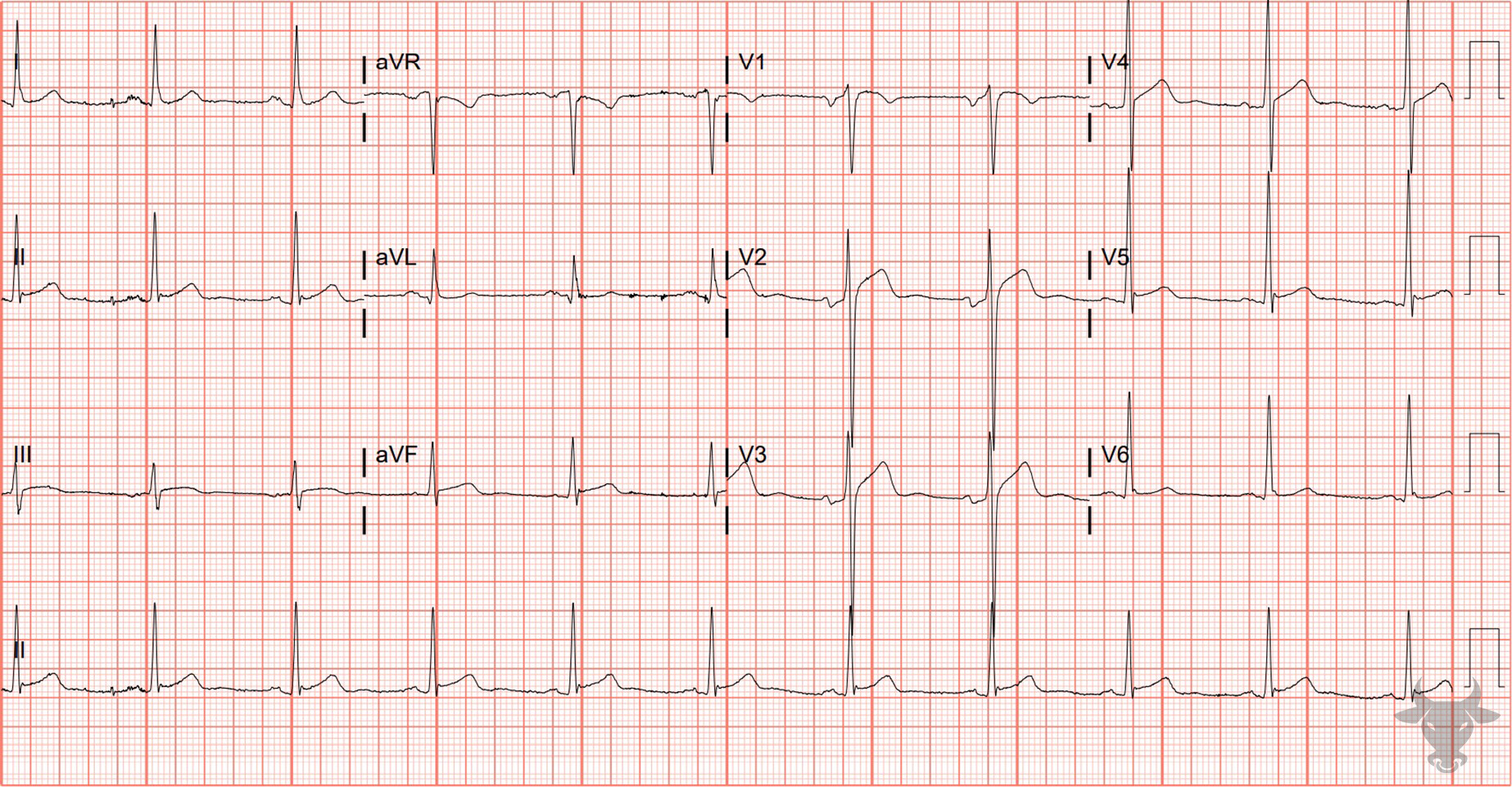
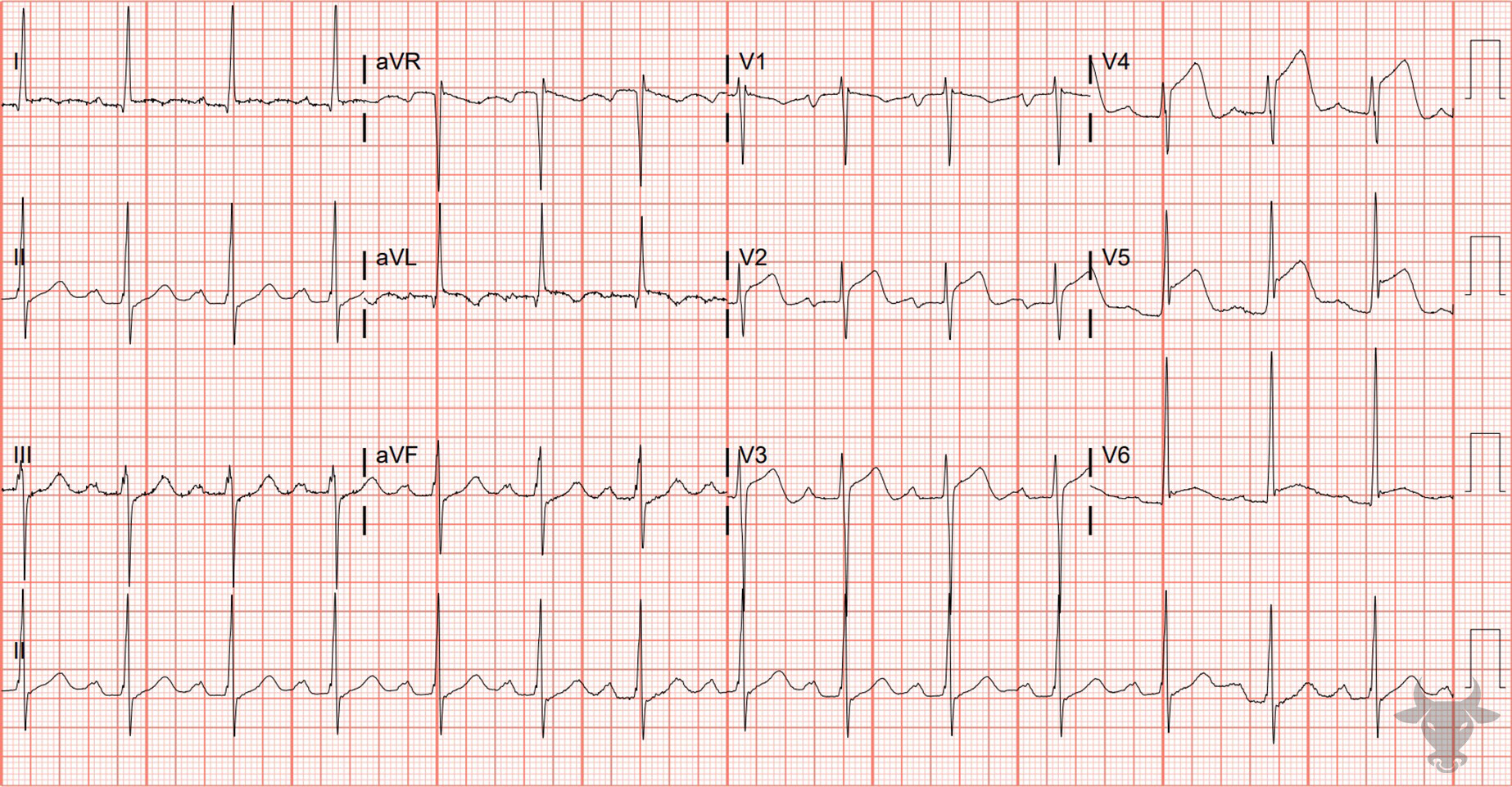
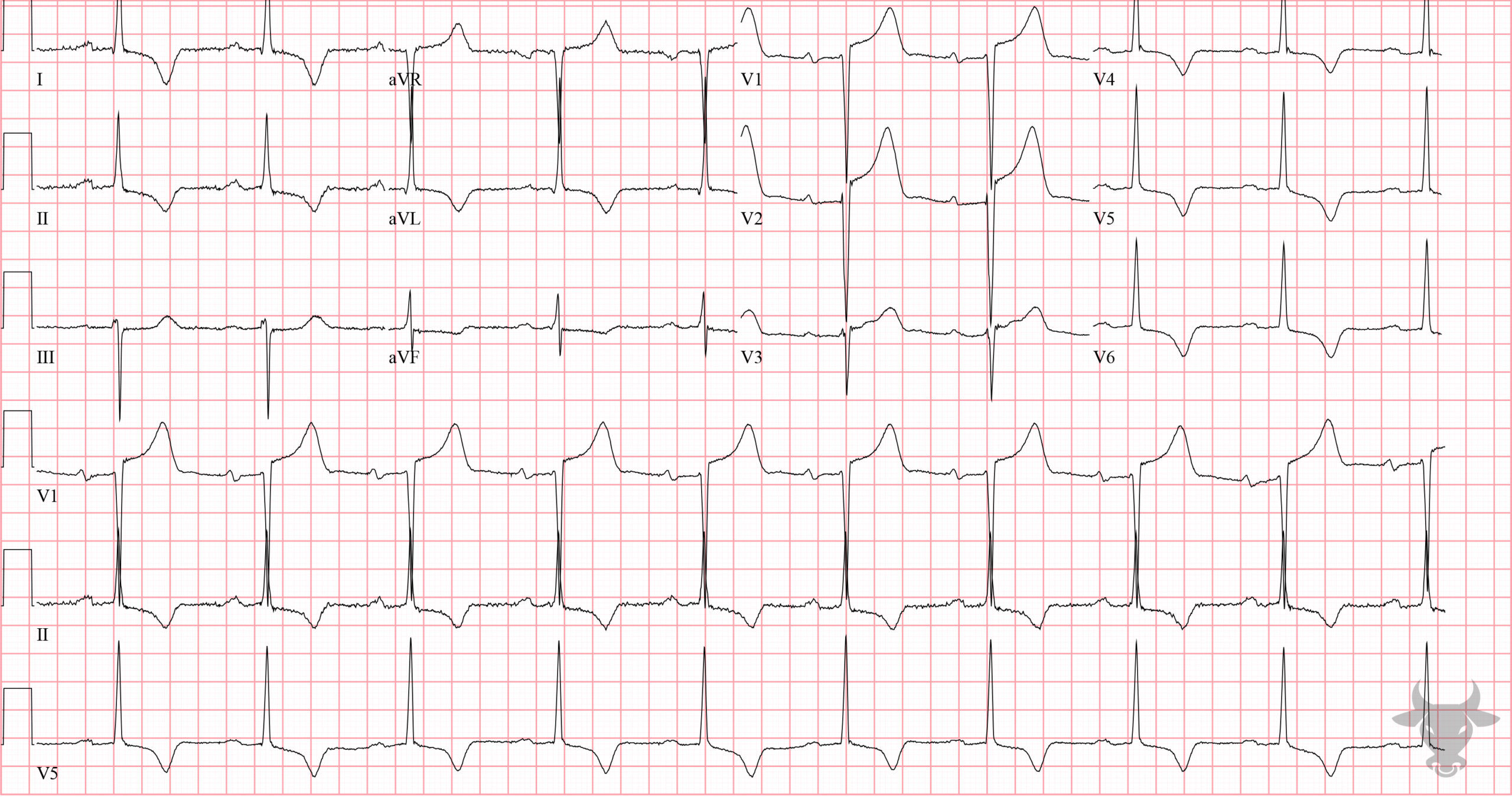
Left ventricular hypertrophy is one of the most common reasons for false activations of the catheterization lab. It often causes discordant ST-elevation in the anterior precordial leads. Armstrong, et al., proposed an algorithm for interpreting acute myocardial infarction in the setting of hypertrophy. Specifically in leads V1 through V3, ST-elevation greater than 25% of the R-S amplitude is likely to be an acute myocardial infarction.