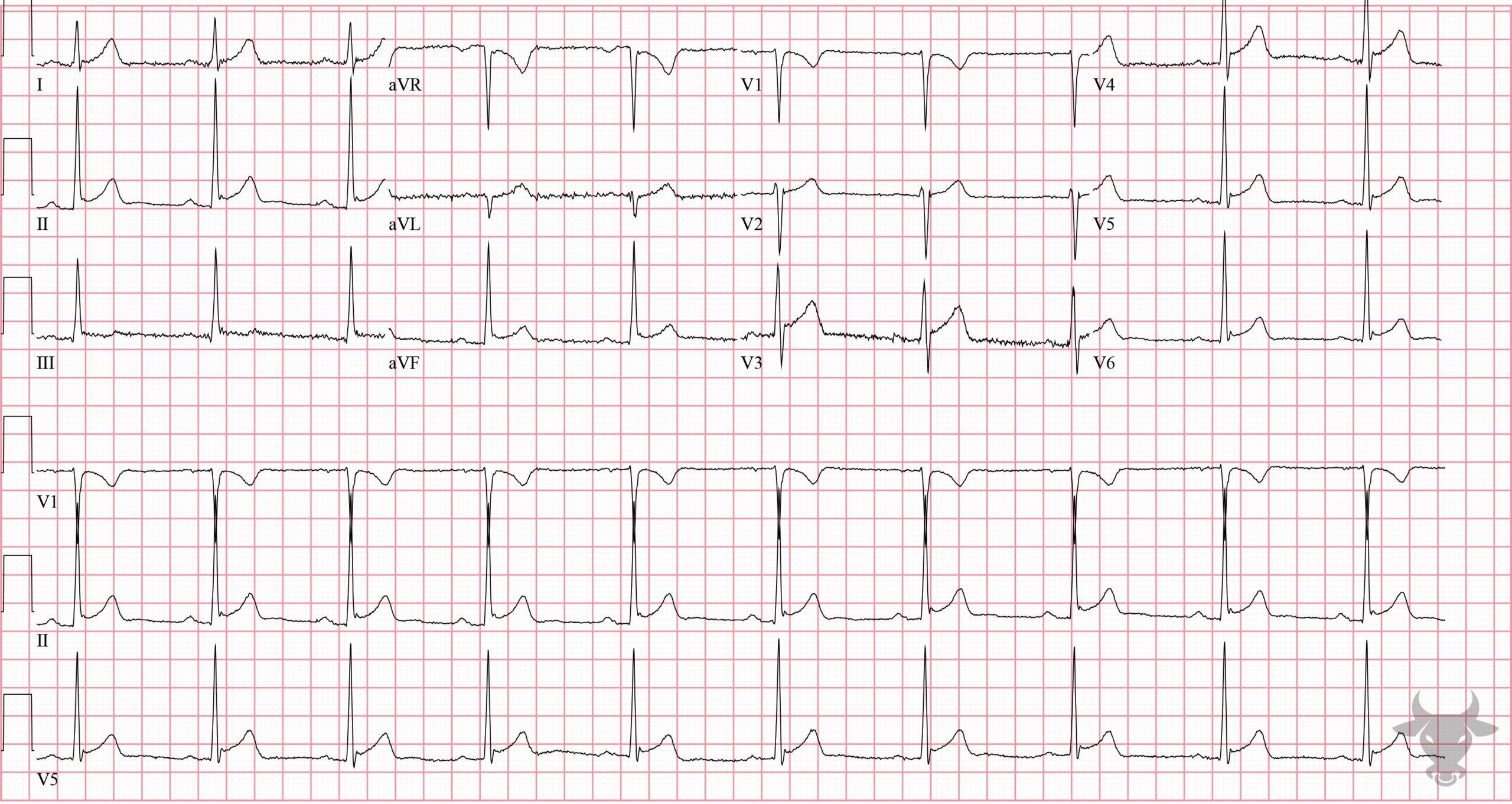
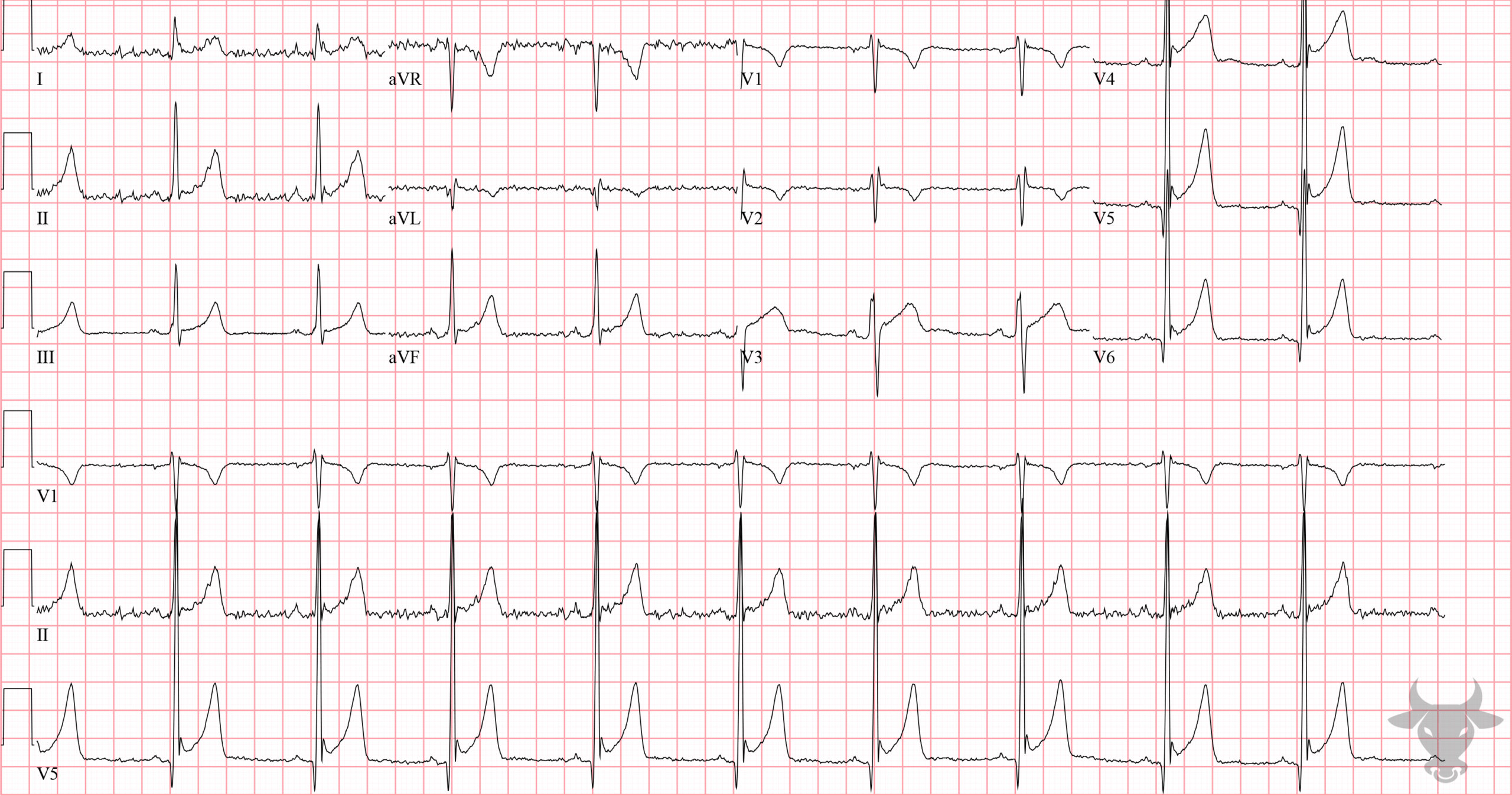
Electrocardiographic features of early repolarization include diffuse ST elevations that are most pronounced in the precordial leads (typically V2-5) and in proportion to the amplitude of the QRS complex. The degree of ST elevation in V6 should be less than 25% the height of the QRS (greater than 25% suggests pericarditis). J point notching (i.e., “fishhook”) can be seen. The T waves should be concordant (same direction as QRS), and there should not be any reciprocal changes to suggest myocardial infarction. When the diagnosis is in doubt, a calculator to help differentiate early repolarization from a subtle anterior ST-elevation myocardial infarction may be useful.
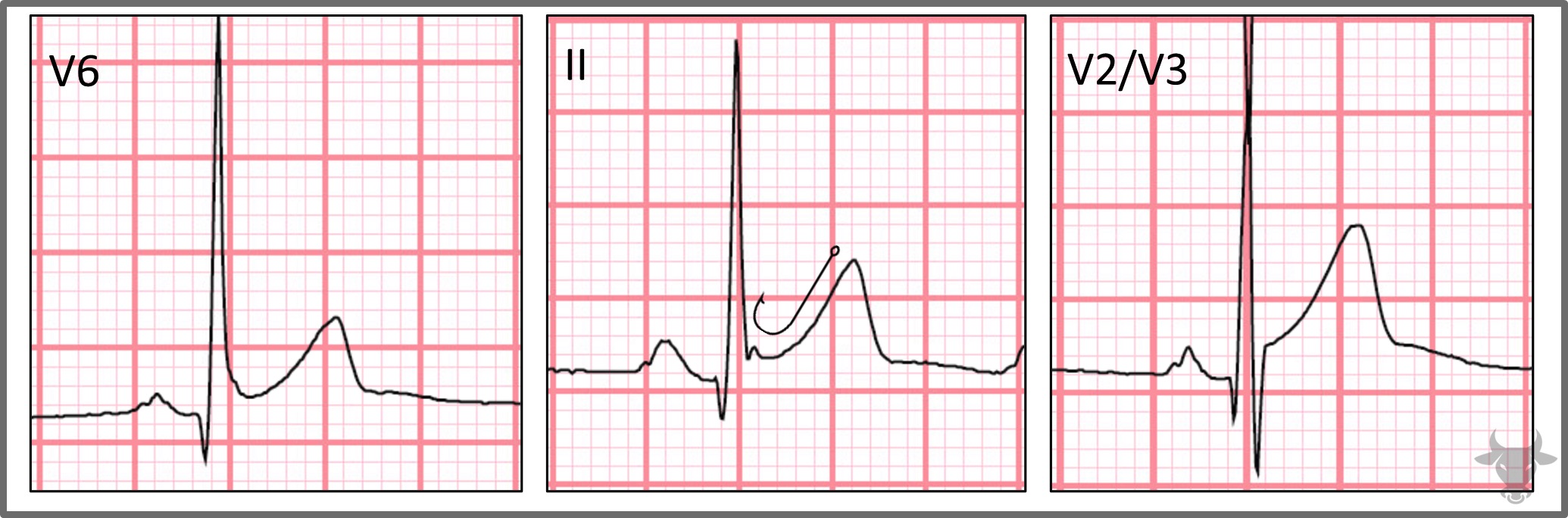
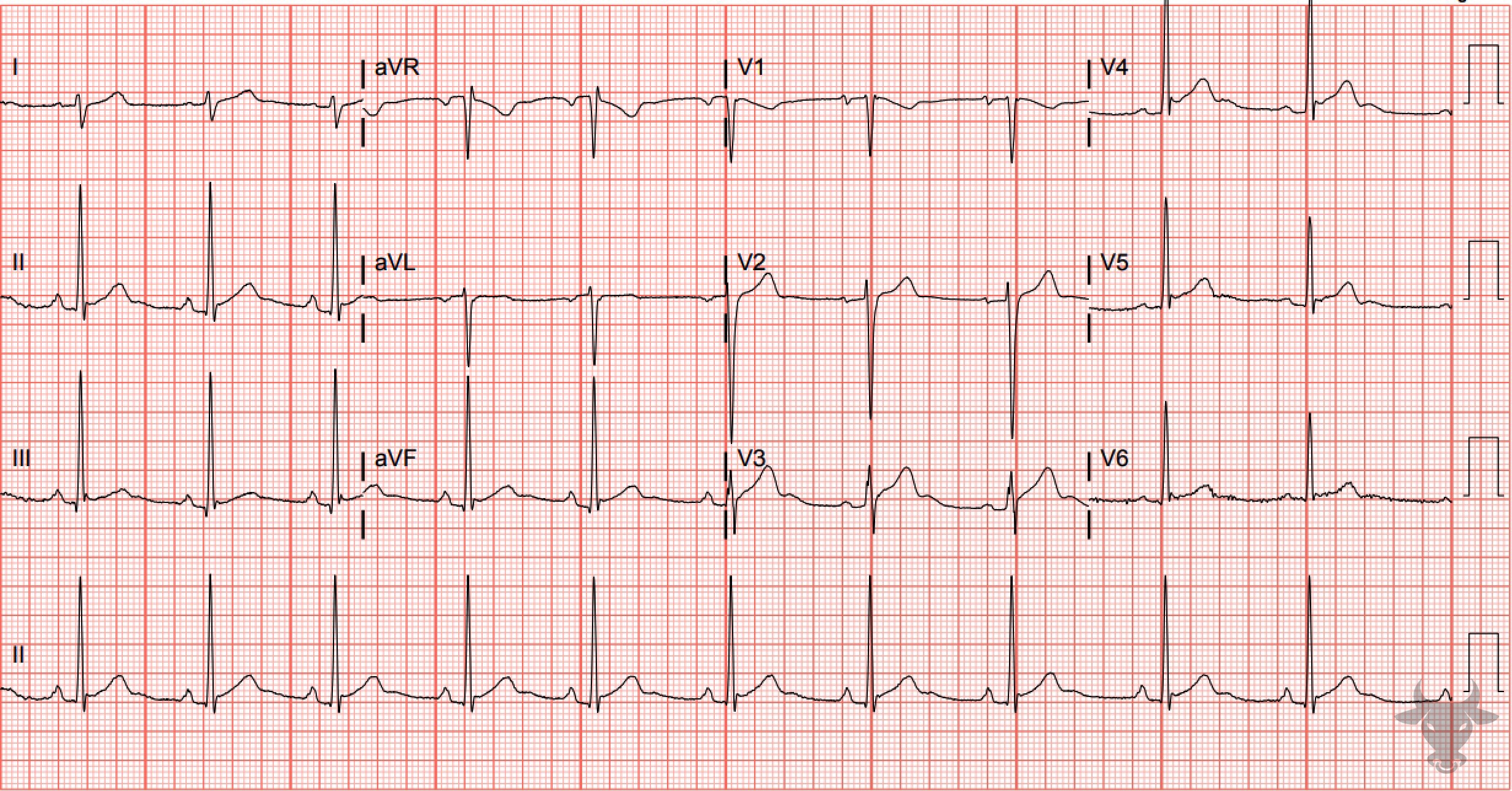
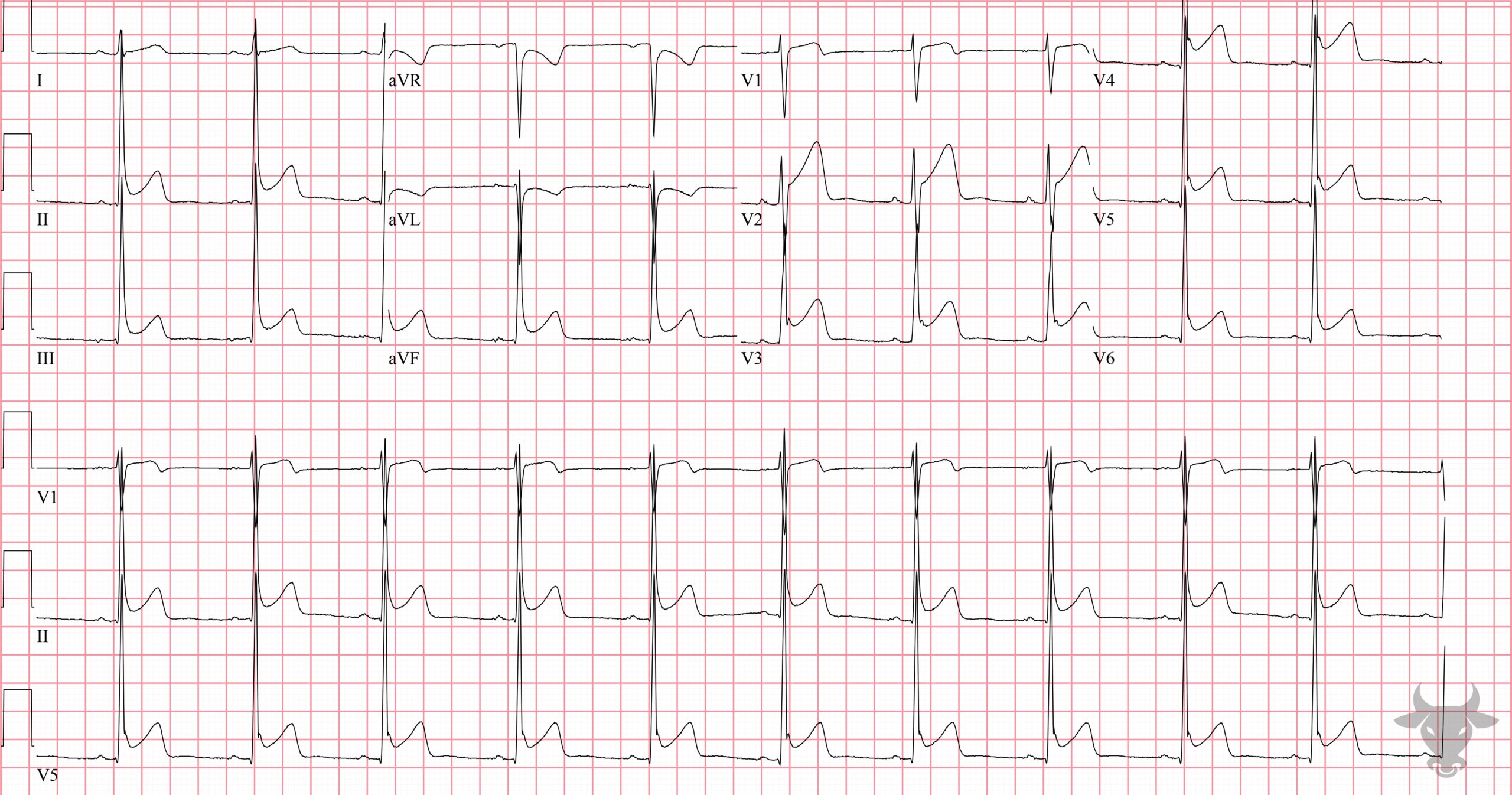
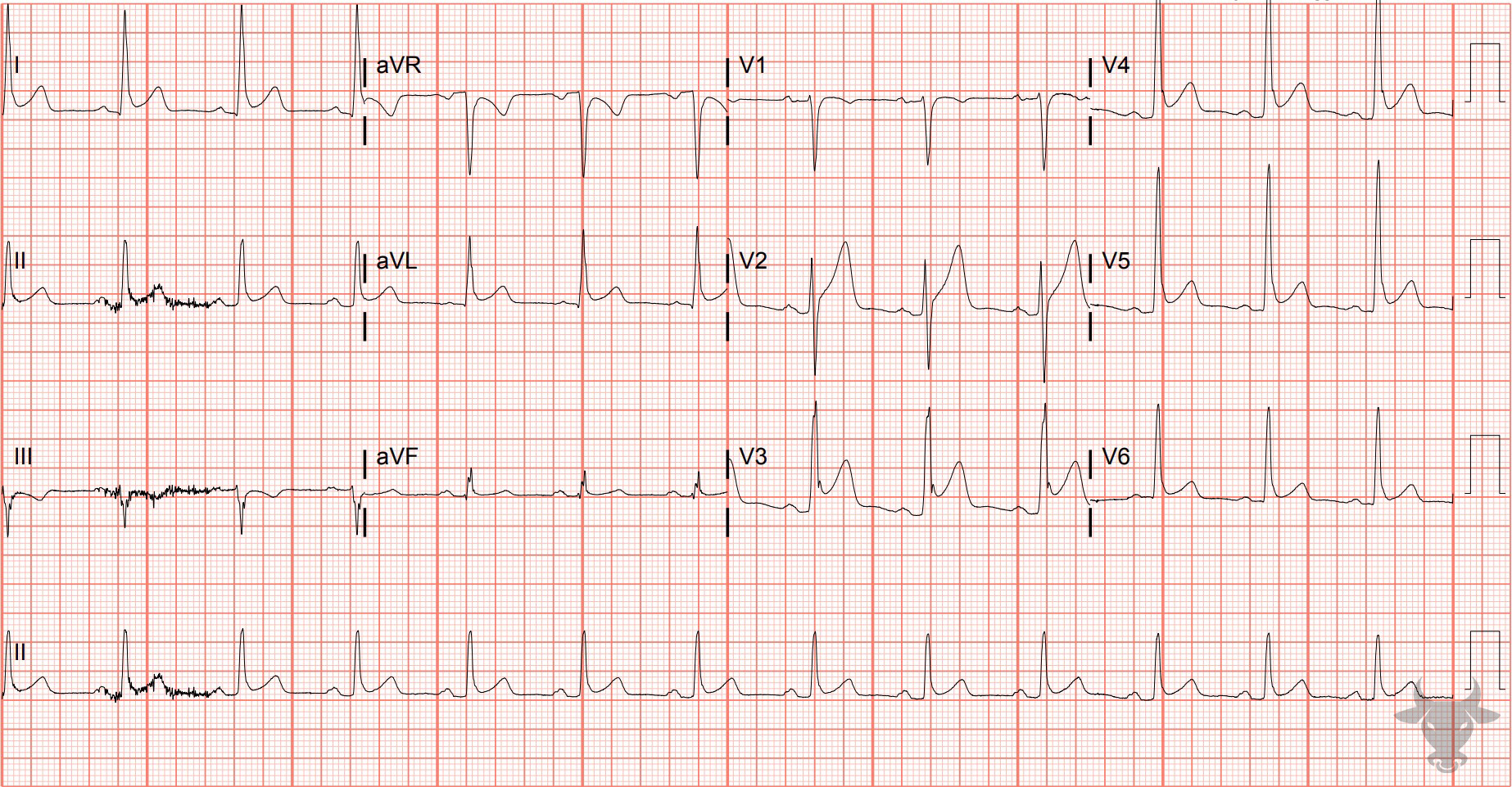
ST elevation can be clearly seen in the above leads. Lead II has J point notching (i.e., “fishhook”), characteristic of early repolarization.