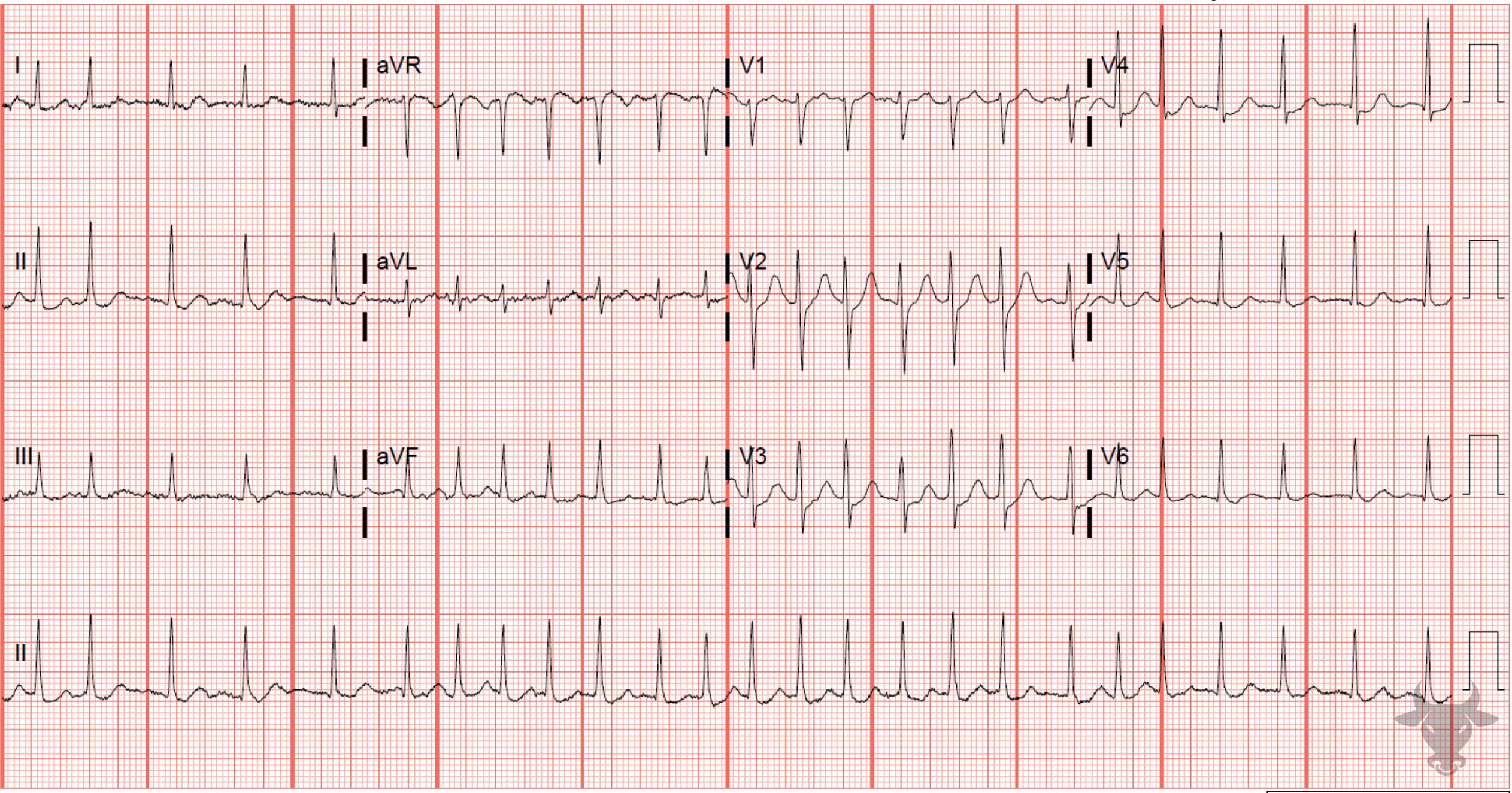
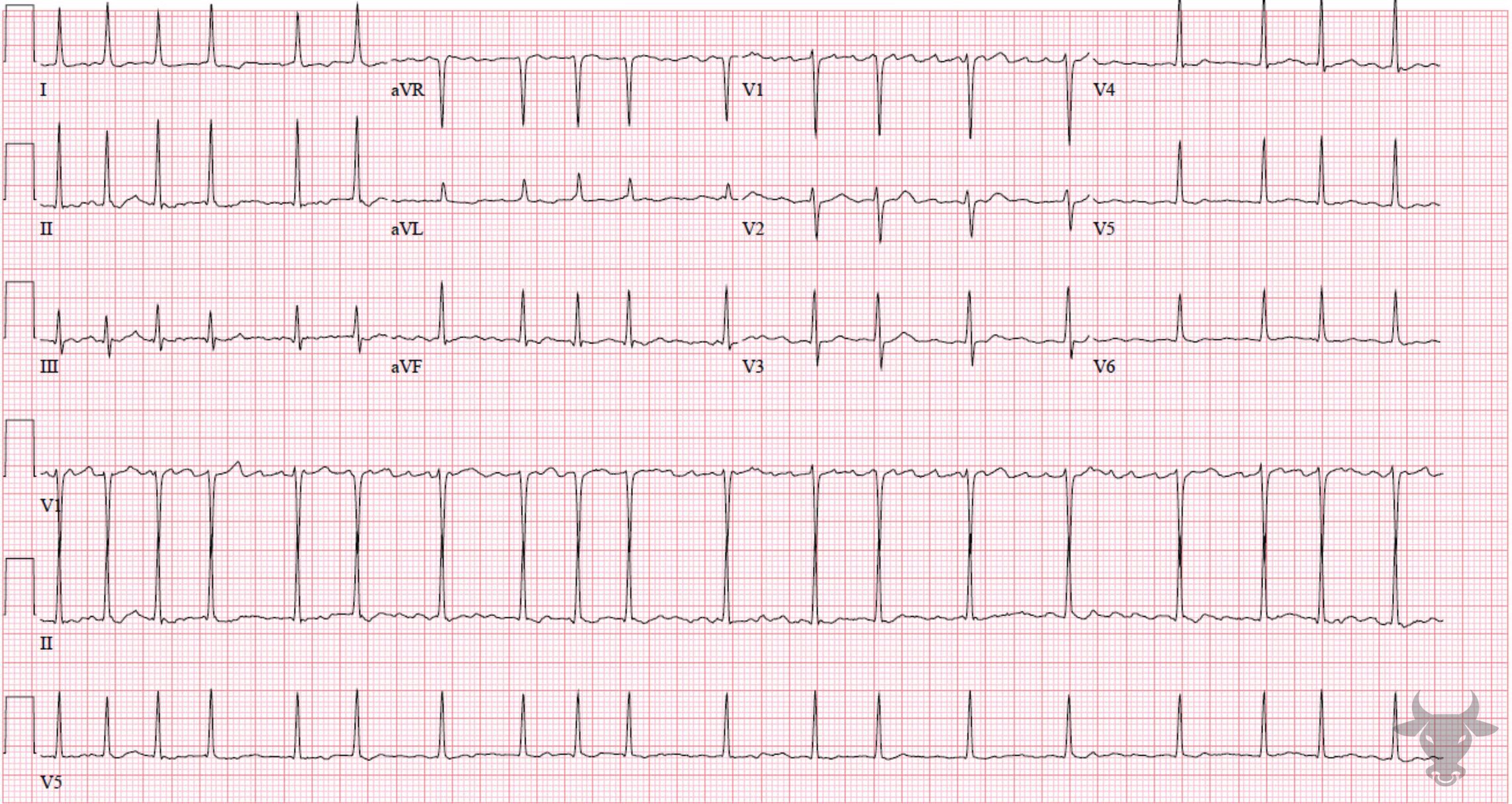
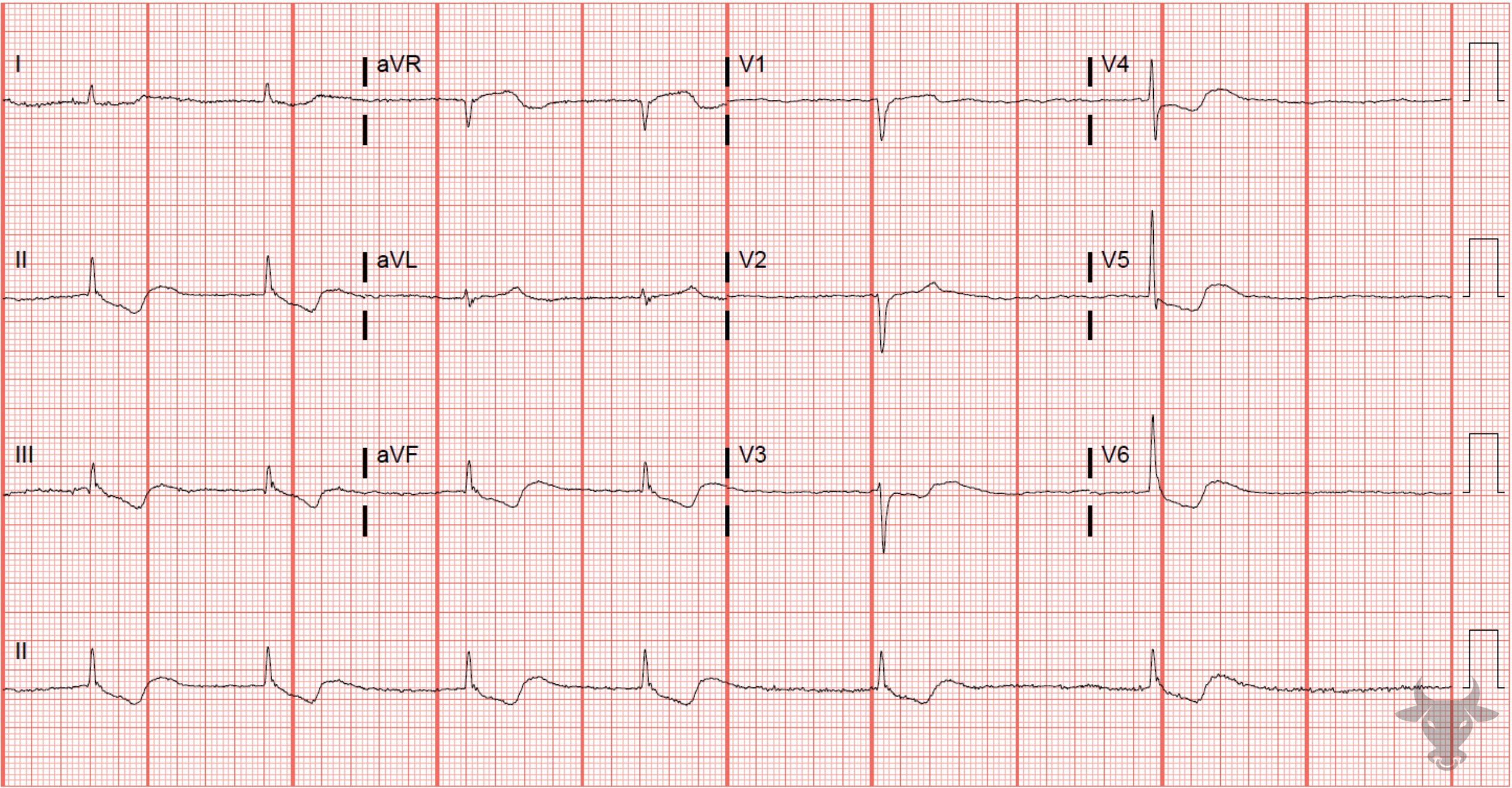
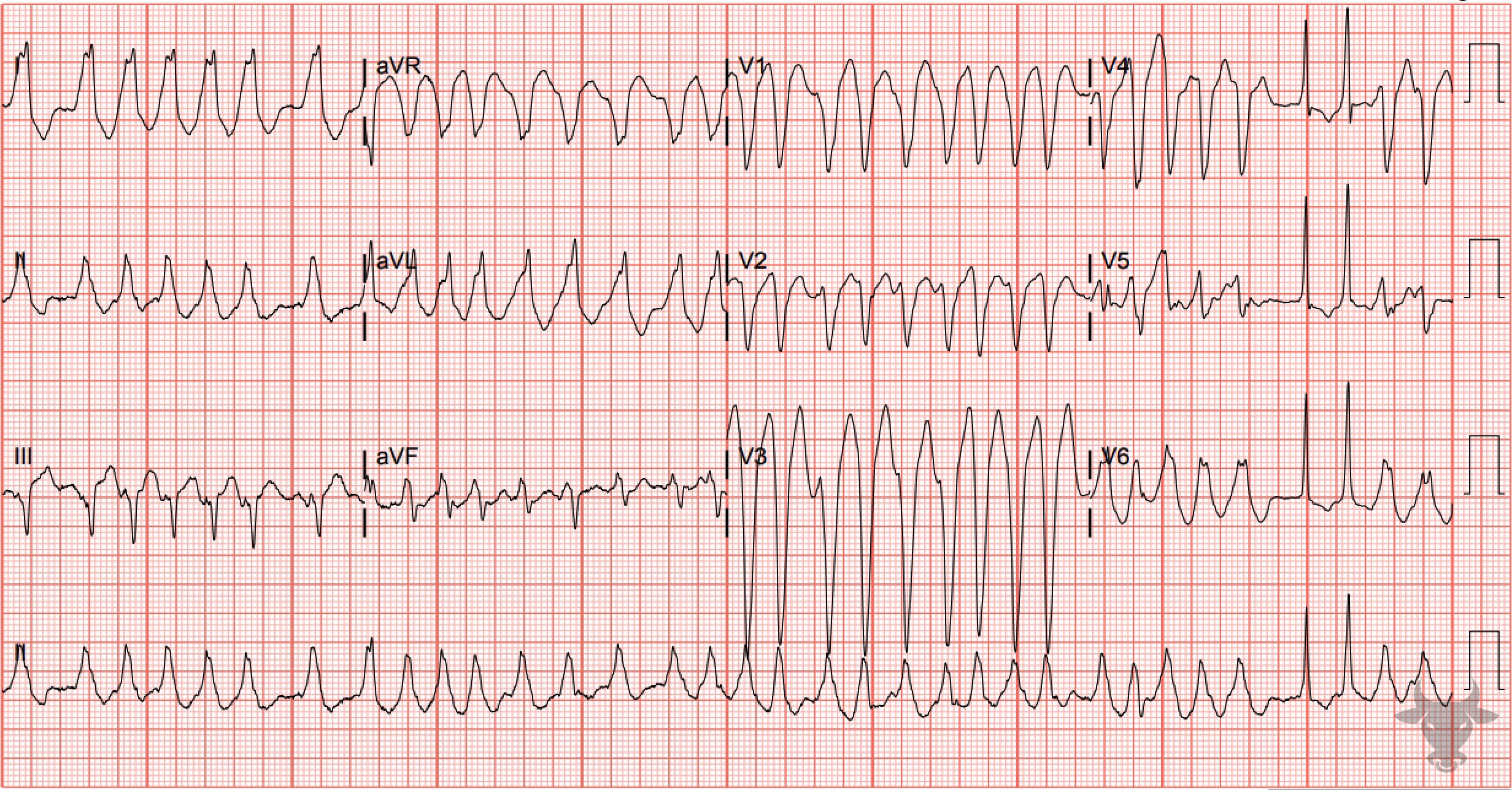
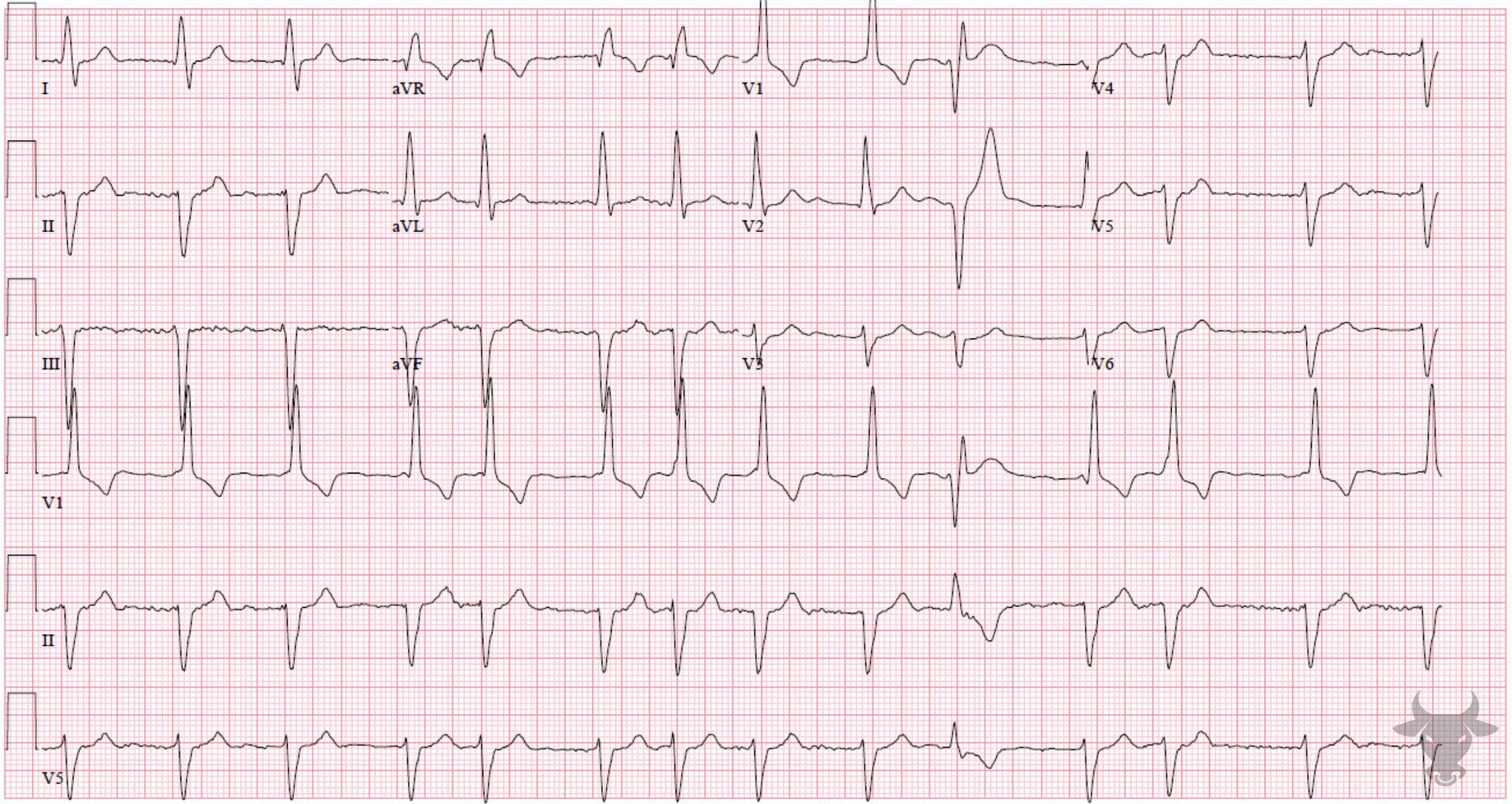
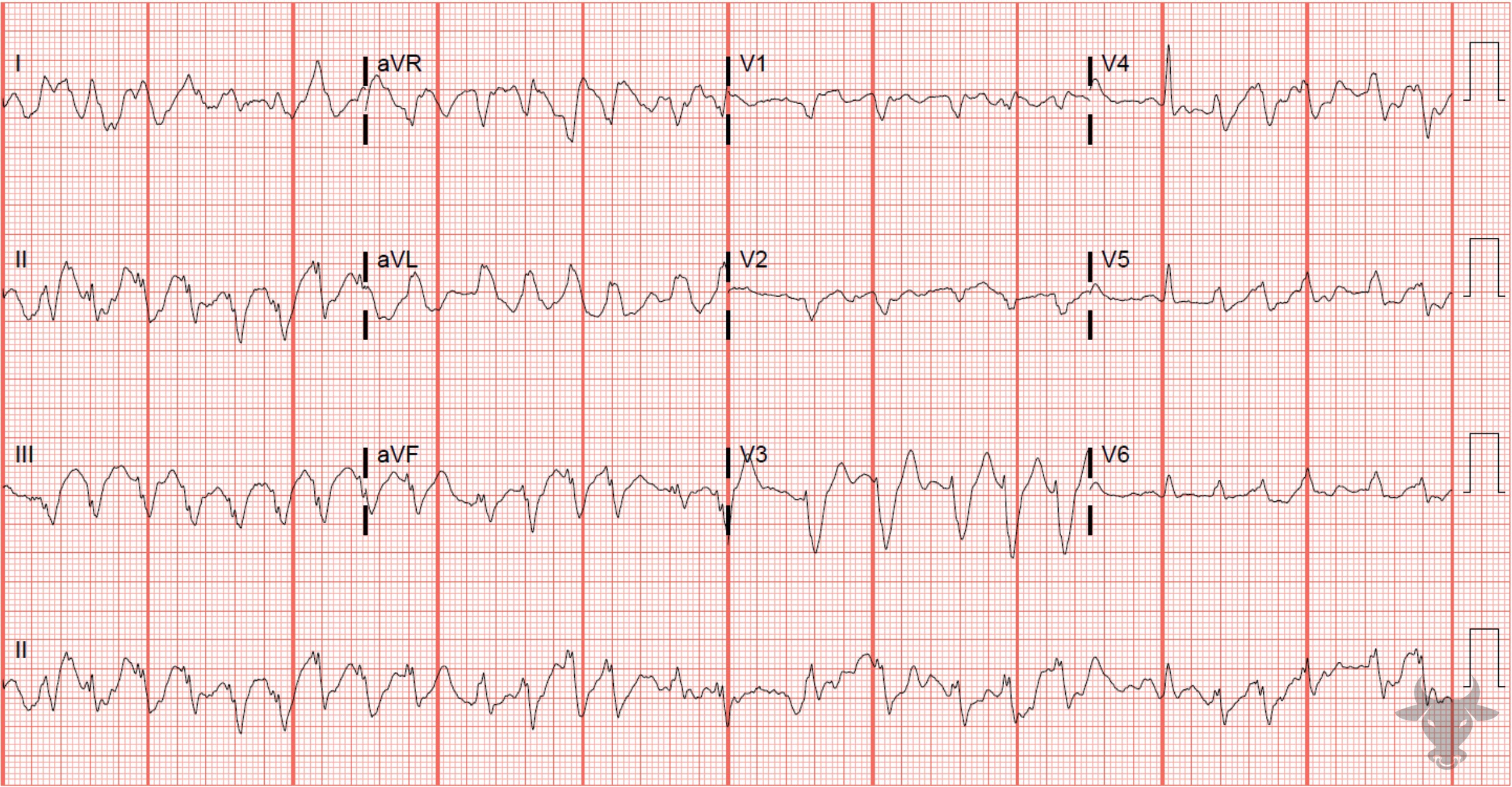
Atrial fibrillation occurs when the atria fibrillate and send rapid impulses to the atrioventricular node. The atrioventricular node serves as the “gatekeeper,” deciding which signals get through to the infranodal conduction system. It causes an irregularly irregular rhythm, the differential of which includes includes atrial fibrillation, multifocal atrial tachycardia, and atrial flutter with variable conduction. Causes include any disturbance of atrial architecture (e.g., inflammation, fibrosis, hypertrophy) increases susceptibility. These changes occur most commonly in the setting of heart disease associated with hypertension, coronary artery disease, valvular heart disease, cardiomyopathies, and heart failure (which tend to increase left atrial pressure and alter wall stress). Extracardiac factors that promote atrial fibrillation include sleep apnea, obesity, alcohol/drugs, and hyperthyroidism.
“Lone AF” is a historical descriptor that has been variably applied to younger persons without clinical or echocardiographic evidence of cardiopulmonary disease, hypertension, or diabetes mellitus. If the duration of onset is reliably less than 48 hours, it is reasonable to offer the patient a rhythm control strategy – either pharmacologic with amiodarone, dofetilide, flecainide, ibutilide, propafenone, or procainamide, or electrical cardioversion. If the onset is longer than 48 hours, pursue a rate control strategy with either beta blockers or non-dihydropyridine calcium channel blockers as first line agents with a heart rate goal of < 110 bpm.
Also, consider anticoagulation after risk stratification with the CHADSVASC score for stroke prevention. Always consider secondary causes of atrial fibrillation (i.e., sepsis, pulmonary embolism, etc.) prior to pursuing a rate control strategy as the heart rate could be compensatory.