Normally, the atrioventricular node serves as the “gatekeeper” for signals arising from the atria – it has a refractory period that does not allow ventricular rates much faster than about 190. Accessory pathways have short refractory periods; therefore, signals can be transmitted at much faster rates with R-R intervals as low as 200 ms (i.e., 300 bpm). Patients with WPW and atrial fibrillation are at risk for deterioration and should be cardioverted. Procainamide or electrical cardioversion are the best options. Atrioventricular nodal blocking agents (e.g., beta blockers, adenosine, non-dihydropyridine calcium channel blockers, digoxin) should be avoided. If the atrioventricular node is blocked, the fibrillatory atrial signals will be transmitted indiscriminately via the accessory pathway, precipitating ventricular fibrillation.
Atrial Fibrillation with WPW

Examples
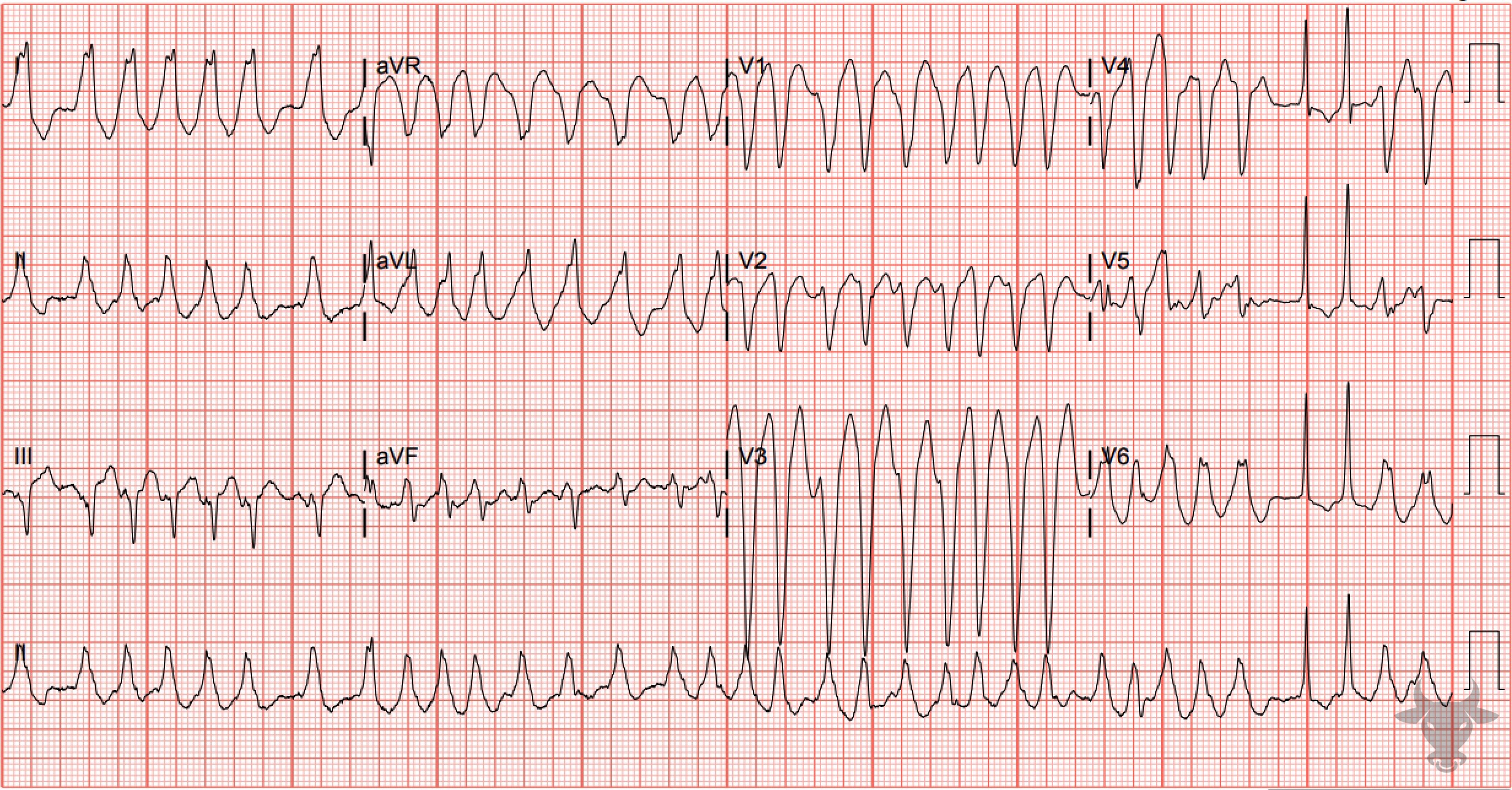
Atrial Fibrillation with WPW
Note the inconsistent QRS morphologies owing to variable transmission of signals from the atria to the ventricles via anterograde conduction through the atrioventricular node and the accessory pathway. The rate approaches 300 bpm at times. Rates this fast are not seen with atrial fibrillation unless an accessory pathway exists. This patient was electrically cardioverted.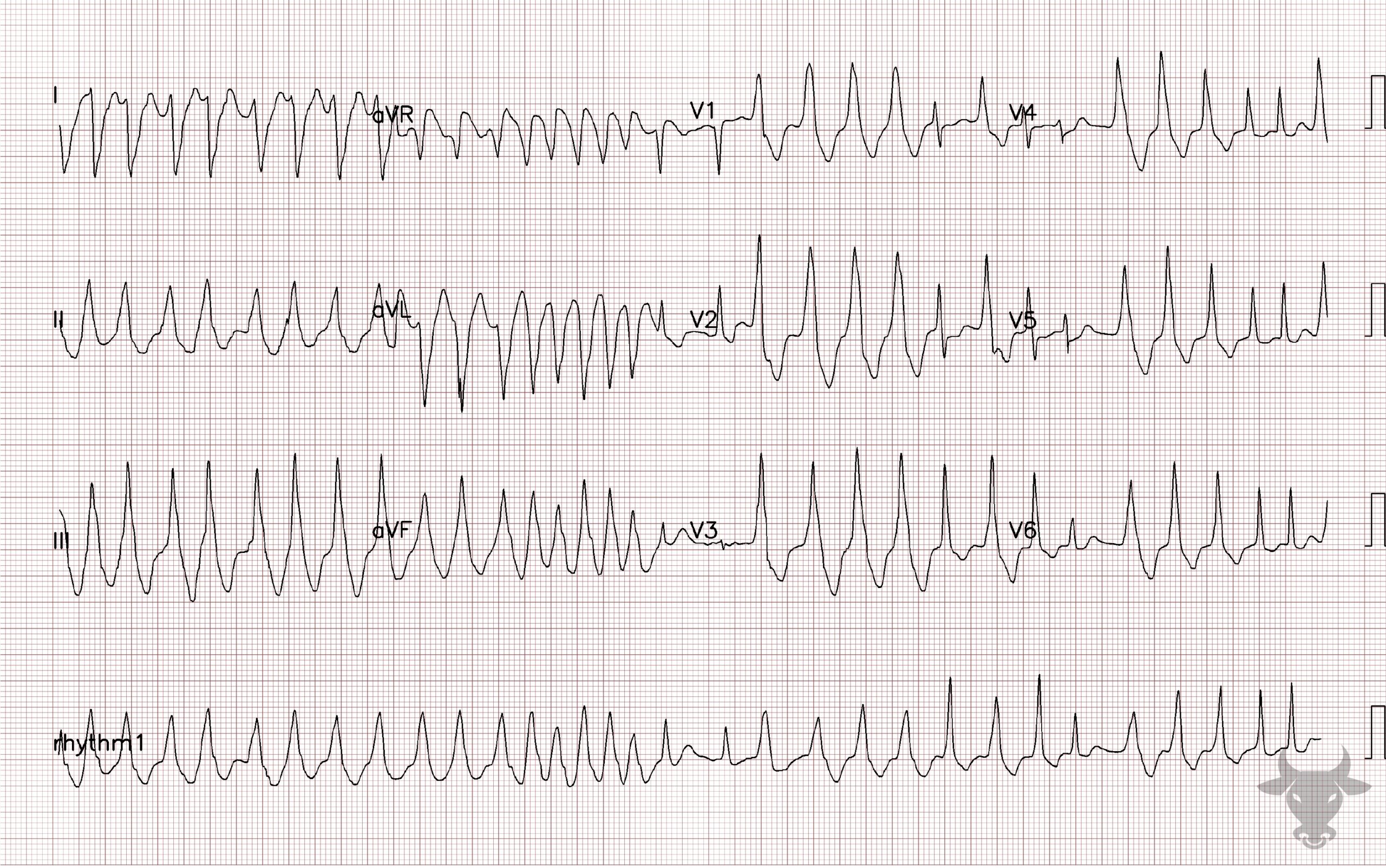
Atrial Fibrillation with WPW
Note the inconsistent QRS morphologies owing to variable transmission of signals from the atria to the ventricles via anterograde conduction through the atrioventricular node and the accessory pathway. The rate approaches 300 bpm at times. Rates this fast are not seen with atrial fibrillation unless an accessory pathway exists. This patient was electrically cardioverted.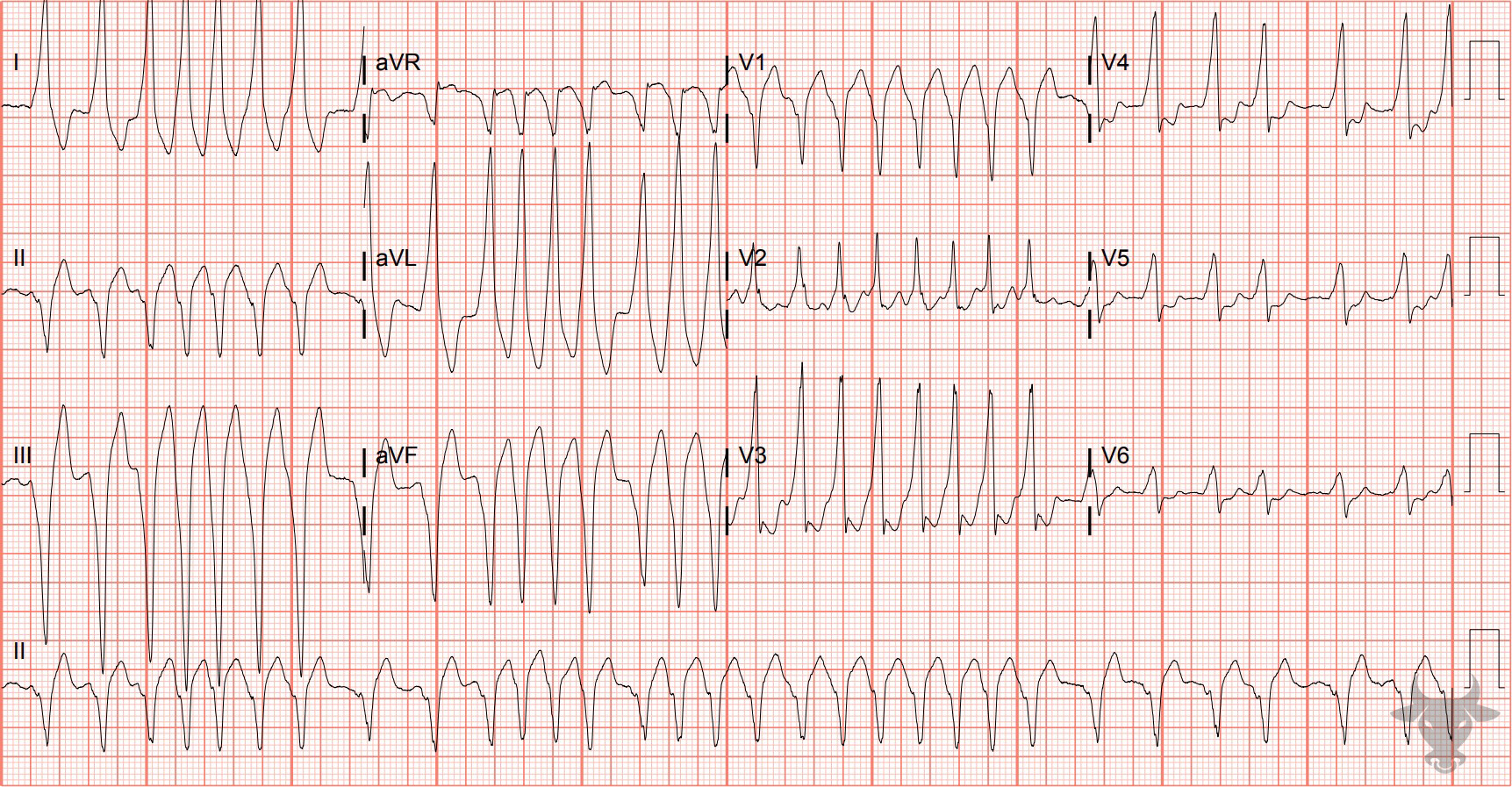
Atrial Fibrillation with WPW
Notice the more-rapid-than-usual rate for atrial fibrillation and changing QRS morphologies consistent with pre-excitation (i.e., Wolf-Parkinson-White). This patient was electrically cardioverted and admitted for a successful accessory pathway ablation.References
- Link MS. Evaluation and Initial Treatment of Supraventricular Tachycardia. New England Journal of Medicine. 2012;367(15):1438-1448.
- Wagner GS, Strauss DG. Marriott’s Practical Electrocardiography. 12th ed. Lippincott Williams & Wilkins; 2014.