The diagnosis is made by meeting 2 of 4 criteria:
- Typical symptoms (pleuritic, sharp chest pain relieved when leaning forward)
- New pericardial effusion
- Presence of friction rub
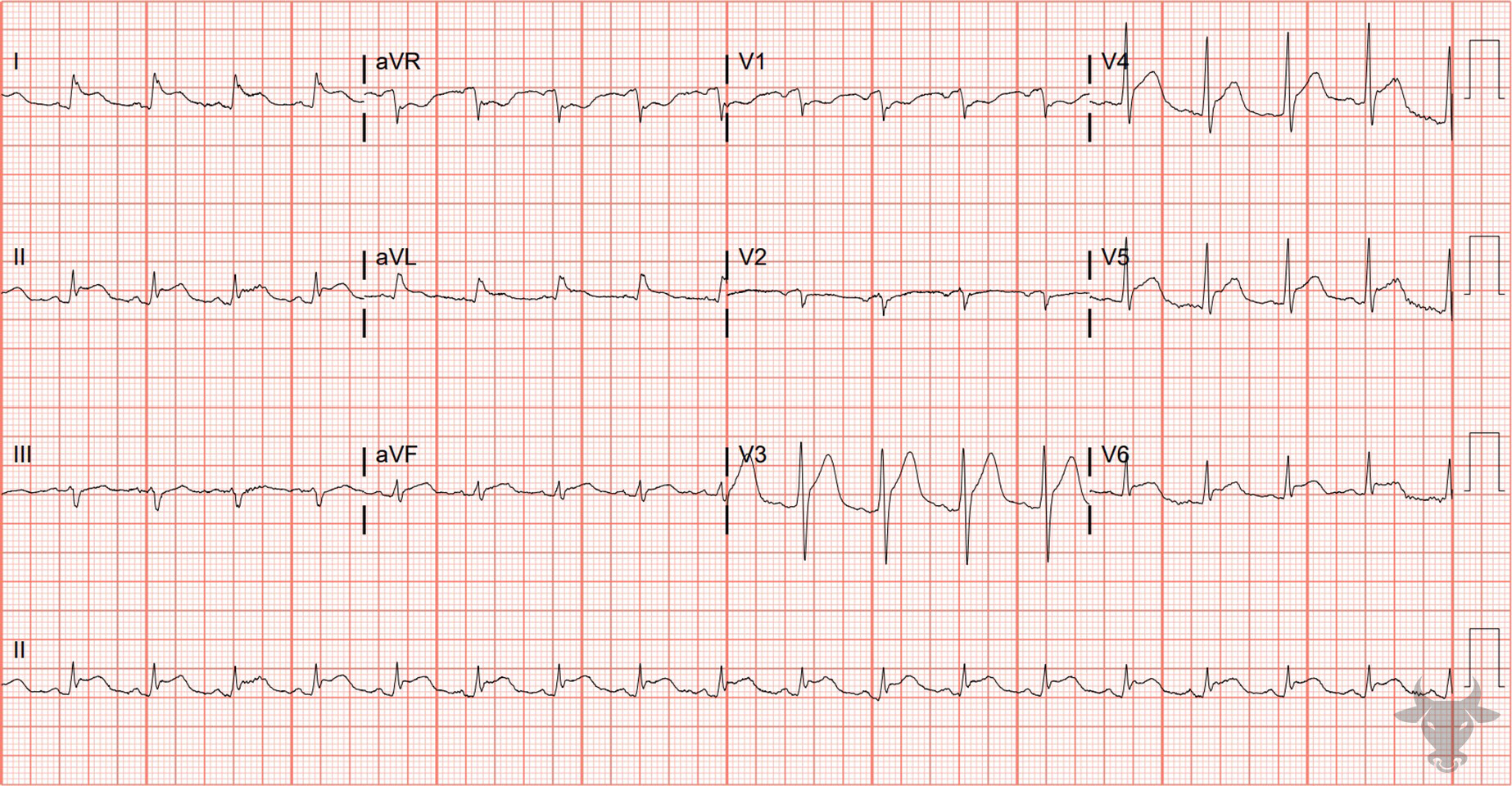
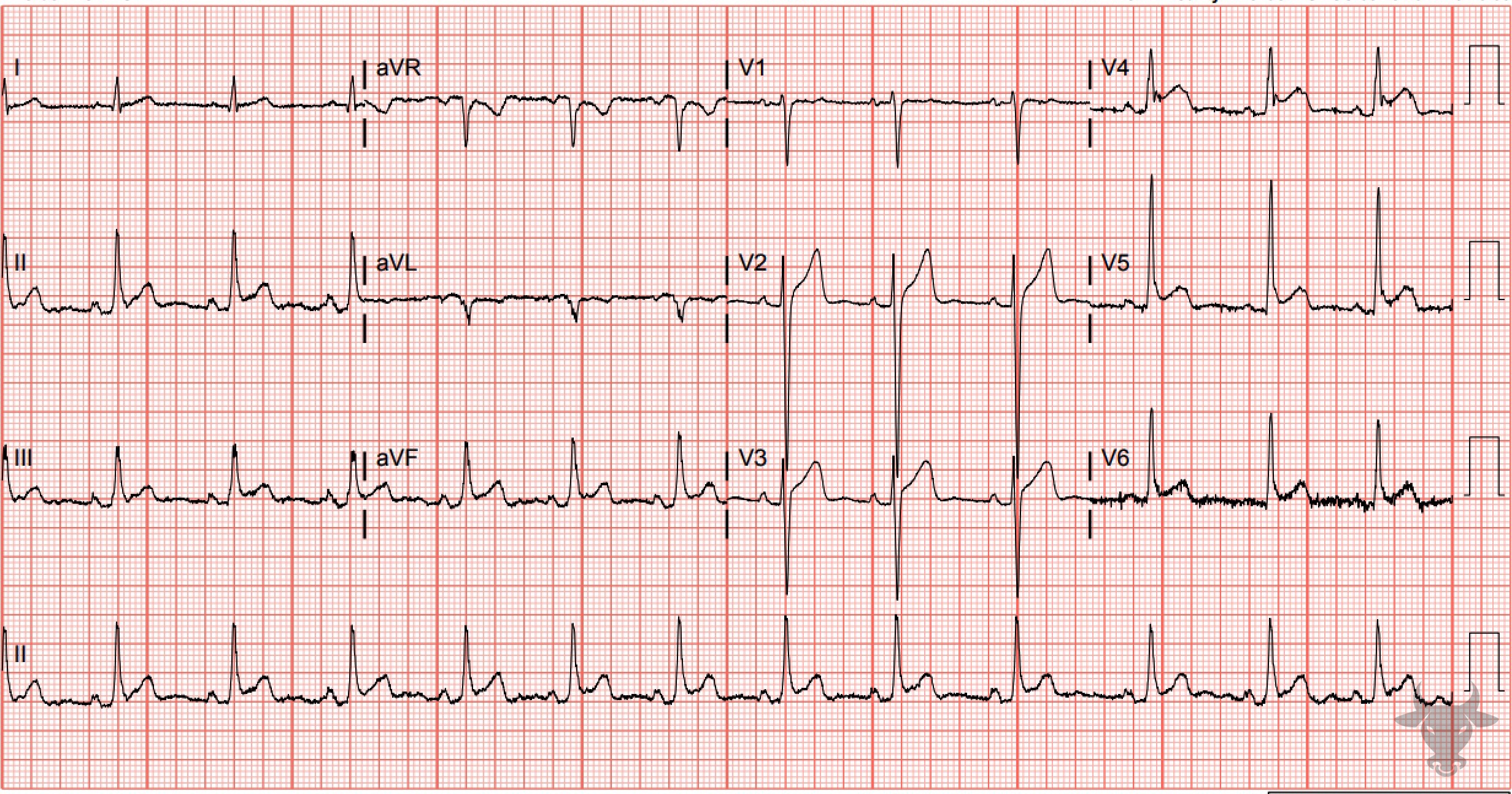
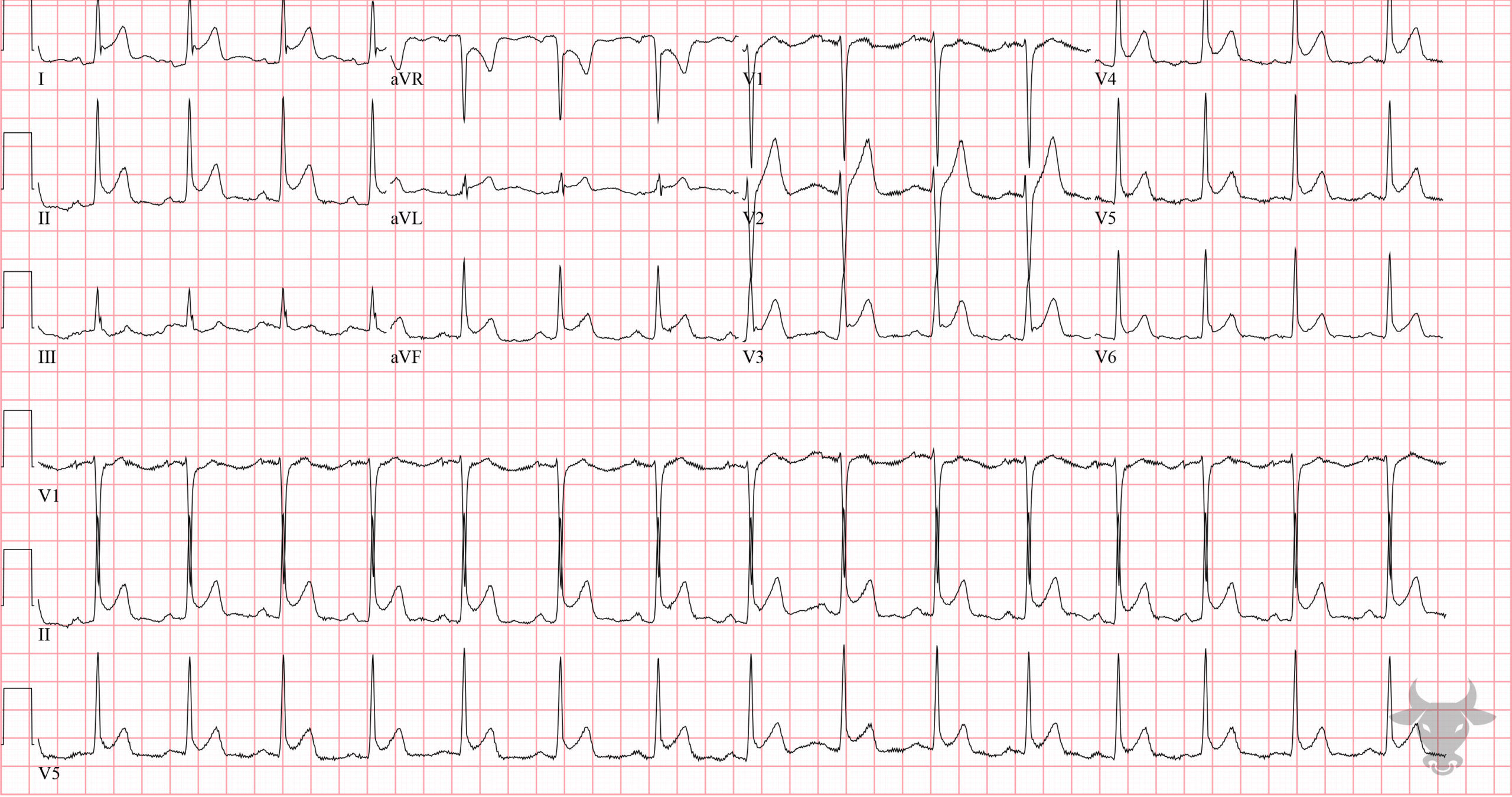
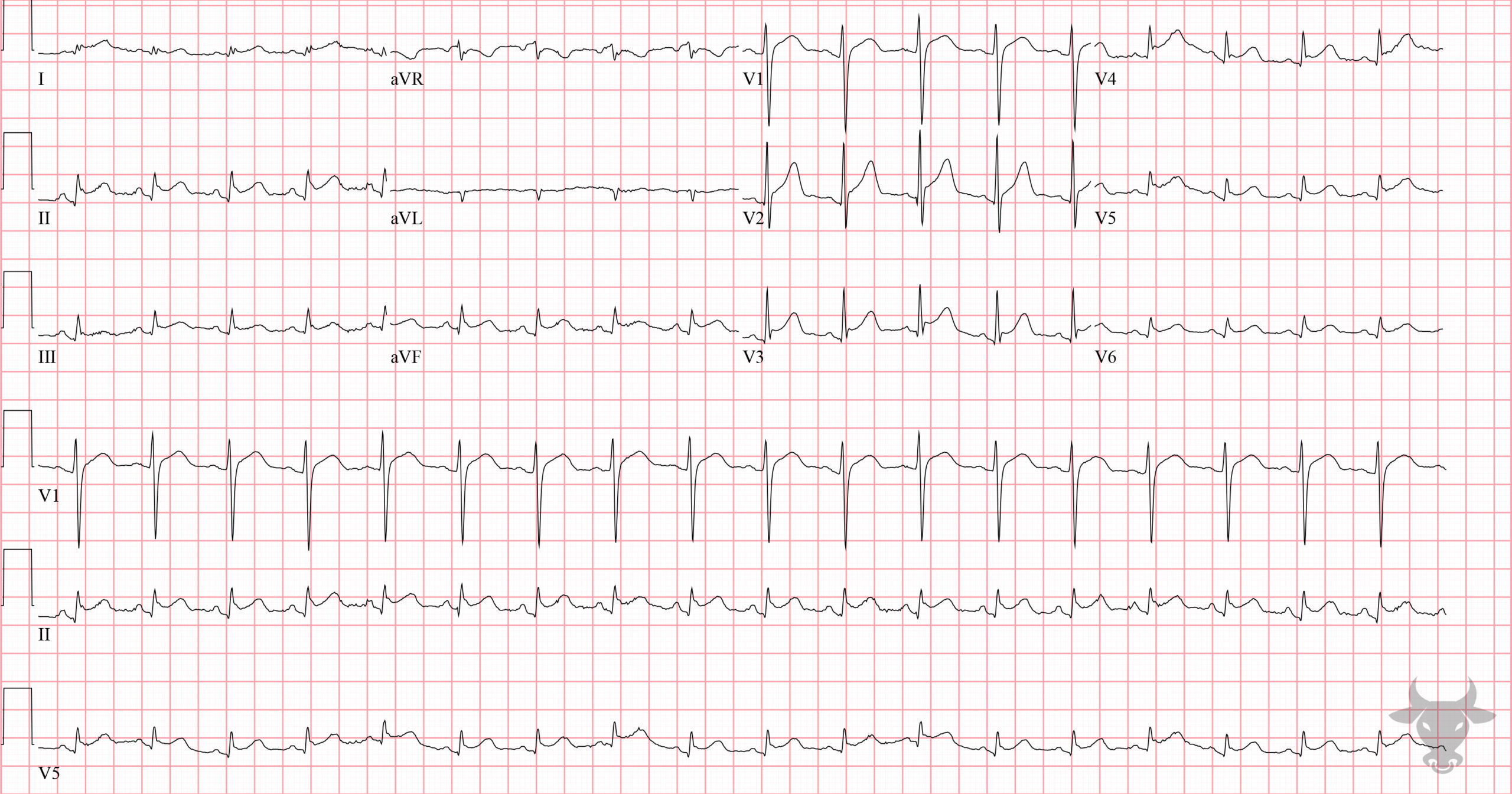
- Typical ECG findings
Differentiating pericarditis from STEMI can be challenging, but features that suggest pericarditis over STEMI include any of the following: diffuse concave up ST elevations without reciprocal changes, PR depression, PR elevation in aVR, ST-elevation in lead II greater than lead III, and Spodick’s sign – down-sloping of the TP segment. It is important to note that the test characteristics of any single electrocardiographic feature is insufficient to rule in/out pericarditis, and that the feature with the highest odds ratio for predicting STEMI is reciprocal ST-depressions.