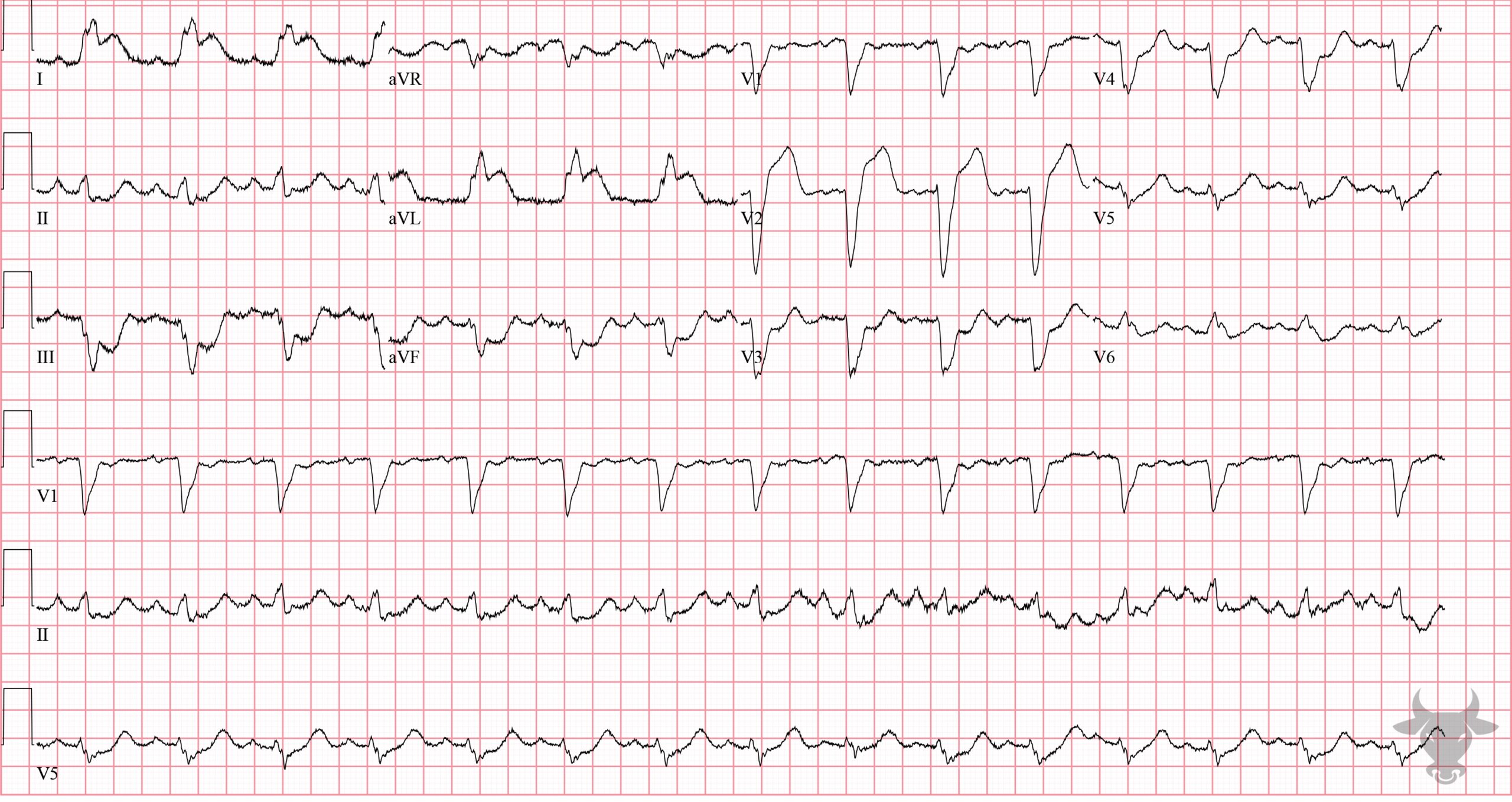
With left bundle branch block, expected ST/T changes include discordant ST depression and T wave inversion in the lateral leads (I, aVL, V5, V6). Discordance describe ST deviation in the opposite direction of the QRS complex (i.e., ST depression in leads with up-going QRS complexes and ST elevation in leads with down-going QRS complexes).
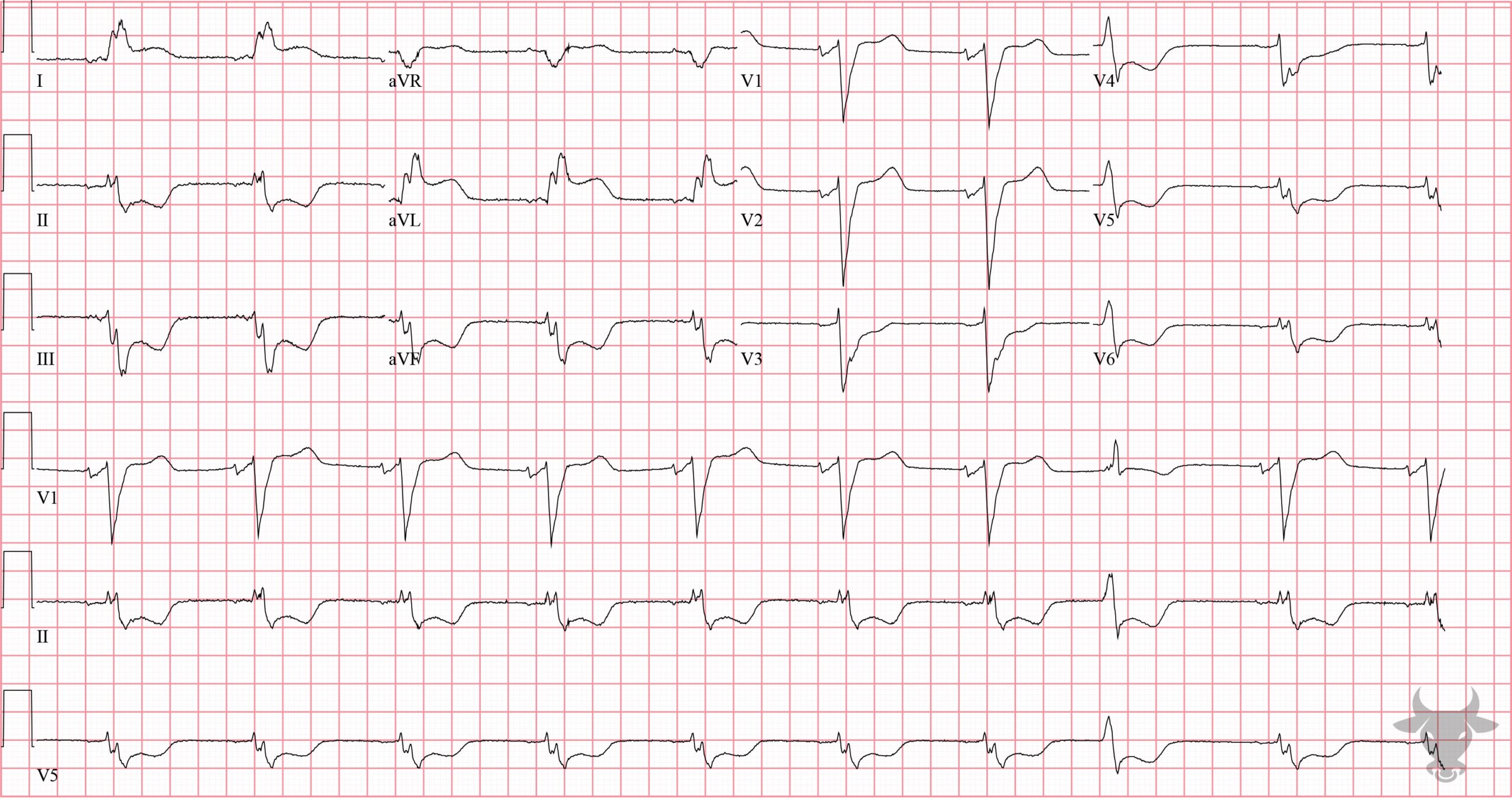
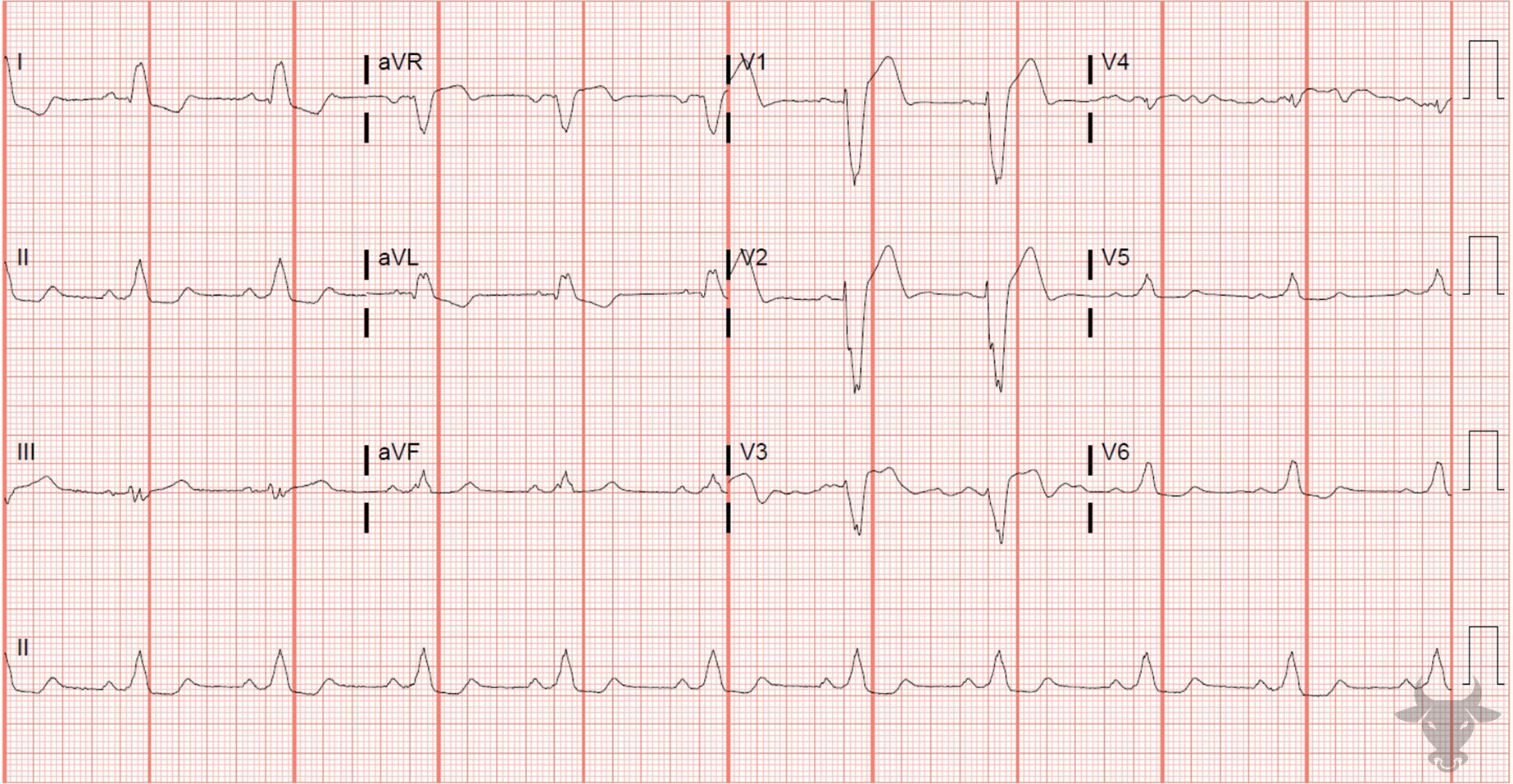
The Sgarbossa criteria are a set of rules to help identify acute myocardial infarction in the setting of a left bundle branch block. The original criteria are:
- Concordant ST elevation ≥ 1 mm
- Concordant ST depression ≥ 1 mm in V1, V2, or V3, or
- Excessively discordant ST elevation (> 5 mm)
The original criteria had a weighting system where excessive discordance was the least specific. The modified Sgarbossa criteria are more sensitive and specific than the original criteria. The first two concordant criteria are the same for the modified Sgarbossa criteria, but the third criterion for excessive discordance takes the concept of proportionality into consideration – excessively discordant ST elevation is defined as an ST/S ratio greater than 0.25.
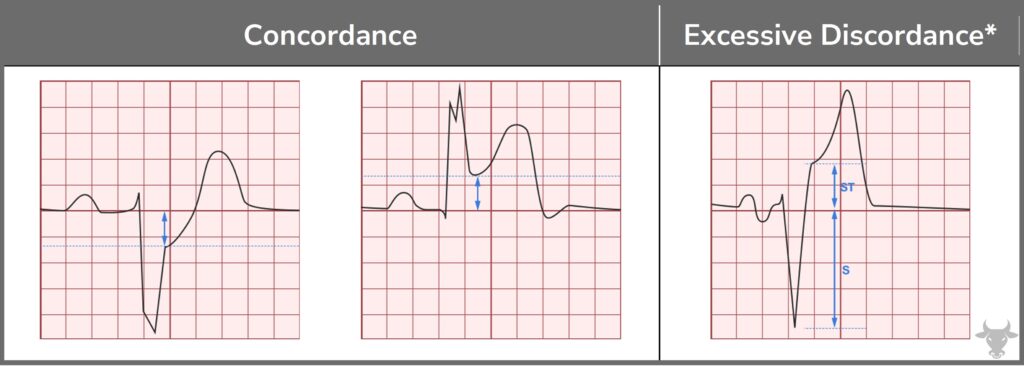
Modified Sgarbossa criteria. ST/S ratio should be greater than 0.25 for excessive discordance.